 History
History
A 44-year-old white male presented complaining of mild watery eyes O.U. that had worsened during the past two months. He also reported that words ran together after prolonged reading.
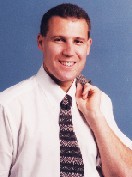
Upon observation, the patient displayed prominent bilateral ptosis. Other notable characteristics included the atypical posture of both eyelids and an expressionless appearance or affect.
When questioned about the droopy eyelids, the patient reported he had been that way since he was a child, and that his father and sister also had droopy eyelids. There were no records available from previous exams.
His medical history was positive for erectile dysfunction, acid reflux disease and chronic sinusitis, for which he was being medicated with Allerest (pseudoephedrine HCI, Insight Pharmaceuticals) nasal decongestant.
The patient also reported difficulty with writing, gripping and letting go after a handshake. Further questioning revealed that his sister might have had muscular dystrophy, but she died at age 45 before receiving a definitive diagnosis.
Diagnostic Data
His best-corrected visual acuity was 20/40+2 O.D. and 20/40-1 O.S. at distance, and 20/30 O.U. at near. Refraction improved visual acuity to 20/25 O.U. at distance and near.
External examination found normal color, ocular motilities and pupils, with no evidence of anisocoria or afferent pupillary defect.
Confrontation visual field testing revealed a superior defect secondary to the patients ptosis but was otherwise full. Amsler grid revealed no metamorphopsias or scotomas in either eye. The bilateral ptosis measured 7mm O.D. and 6mm O.S. The anterior chambers were deep and quiet. Intraocular pressure measured 12mm Hg O.D. and 11mm Hg O.S.
Your Diagnosis
How would you approach this case? Does this patient require any additional tests? What is your diagnosis? How would you manage this patient? What is the likely prognosis in this case?
Thanks to Caroline Pate, O.D., from the
Discussion
The diagnosis in this case is myotonic dystrophy (MD), the most common adult form of muscular dystrophy. This condition is an autosomal dominant disease that is characterized by myotonia (a slow relaxation of muscles after contraction), muscle weakness and progressive muscle atrophy.1-3
MD can affect multiple systems throughout the body, particularly cardiac, endocrine and respiratory systems. Patients with MD have a shorter life expectancy due to cardiac or pulmonary complications.1,2
The severity of the disease tends to increase with each subsequently affected generation. Decreased intelligence and mental retardation can occur after three to four consecutively affected generations.1,2 Less severe cases may be virtually asymptomatic and are often undiagnosed.1
MD tends to surface between ages 20 and 30, but can occur at any age.1,2 The disease affects all races and sexes equally, with a prevalence of approximately one in 8,000 patients.1,2,8
Ocular complications accompany almost all cases of MD. Patients typically present with cataracts, extraocular muscle involvement, ptosis, hypotony, and macular and retinal pigmentary changes.1-7 Bilateral ptosis, polychromatic lenticular opacities, extraocular muscle involvement, hypotony and macular changes also are typical of MD.
These conditions are often the first clinically diagnostic signs of the disease in otherwise asymptomatic patients. Optometrists and ophthalmologists need to be aware of MD, for the ocular complications associated with this disease are numerous.
We tentatively diagnosed this patient with presumed MD until a neurologist could confirm the diagnosis. We also added bilateral ptosis to the patients assessment list. The patients visual acuity was reduced secondary to the Christmas tree cataracts, 1+ inferior cortical cataracts and trace nuclear sclerosis O.U.
We instructed the patient to wear ultraviolet protective sunglasses when outdoors. We also gave him a home Amsler grid test to administer weekly.
Additionally, we diagnosed the patient with dry eye syndrome O.U., secondary to lagophthalmos, and advised him to use preservative-free TheraTears (Advanced Vision Research) q.i.d. We also discussed lid hygiene with the patient, including lid scrubs O.U. with OcuSoft premoistened wipes and hot compresses b.i.d. O.U. Finally, we prescribed bifocal spectacle lenses to help him read more clearly.
We sent a letter to the patients primary-care physician, in which we reported our findings and our recommendation that the patient undergo a systemic work-up and neurological consultation to confirm the clinical diagnosis of MD. We instructed the patient to return to the office in three months for follow-up.
We requested reports from the neurologist regarding the systemic workup for MD. Thyroid function studies; complete blood count (CBC) with differential; and general chemistry, including random blood glucose and hemoglobin A1C, were all normal. An aceylcholine receptor antibody test ruled out myasthenia gravis. Creatine kinase enzyme testing showed elevated levels at 333 units/L (normal range is 35 to 250 units/L), which signals the presence of muscle injury or disease, as in MD.
The neurologist recommended that the patient undergo electromyography and muscle biopsy at a later date.
The genetic inheritance pattern of MD has been mapped to an expanded CTG (cystosine, thymine, guanine) repeat in the protein kinase gene (DMPK) located on chromosome 19q13.3.3,5,9-11 The length of the expanded CTG repeat tends to increase with successive generations and corresponds to a heightened severity of the disease.1,2,9,12 Normal patients have approximately five to 30 repeats, while those with a mild form of the disease show 50 to 80 repeats; the most severely affected have more than 2,000 repeats of the CTG nucleotide.13 There is great variability in expression of the disease, which accounts for the diverse range of systemic and ocular signs and symptoms.
The systemic manifestations of MD are numerous, including cardiac disease, testicular atrophy, respiratory impairment, hypersecretion of insulin, abnormal carbohydrate metabolism, gastrointestinal abnormalities, frontal baldness, weight loss, and mental disorders, including both mental retardation and depression.1,5 The first muscles often affected in the disease include those of the face, jaw and neck, giving patients the characteristic appearance of a droopy, expressionless face.1,5,8
Besides muscle deterioration, myotonia, or the inability to relax a contracted muscle, is noted in MD patients. Difficulty releasing ones grip after a handshake is a classic example of myotonia. The myotonia experienced by these patients is most often exacerbated by cold, excitement, menses and pregnancy.1,5
Those patients with significant stiffness and trouble relaxing their muscles benefit most from avoiding cold temperatures, performing warm-up exercises, and repetitively using the muscles most often affected. Antimyotonic drugs, such as procainamide and diphenlyhydantoin, may be used in extreme cases to reduce myotonia.1 Later involvement of muscles in MD includes the larynx, pharynx and vocal cords, resulting in slurring of speech, a nasal tone to the voice, and difficulty swallowing.1,8,10
The most noteworthy ocular finding: the polychromatic Christmas tree cataracts, which appear in every patient with MD and are pathognomonic of the disease.1,4,14 The cataracts are typically bilateral and may be cortical, sutural or subcapsular in location.1,2 The lenticular opacities consist of punctate, iridescent, colorful changes that may require extraction if the cataract significantly impairs vision.
There have been isolated reports regarding complications of recurrent posterior capsular opacification, anterior capsulorhexis contracture, and rubeosis irides in patients with MD who undergo cataract surgery.3,15,16 Posterior capsular opacification is not uncommon after cataract surgery, with up to 50% of patients requiring a Nd:YAG laser capsulotomy to restore good visual acuity.16 Five documented cases showed that MD patients with recurrent posterior capsular opacification and anterior capsulorhexis contracture required as many as five capsulotomies.3,16
The etiology of the recurring capsular fibrosis and anterior capsulorhexis contracture in MD patients is believed to be secondary to atrophy in the ciliary body. However, the majority of these patients will only require one laser treatment.16 Genetic studies of the lens epithelial cells in MD patients reveal the presence of the DMPK gene mutation that is characteristic of the disease.16
Regardless of the type of lens implant used, MD patients should be made aware of the possibility of multiple postoperative laser treatments to correct posterior capsular opacification.
Another rare, post-op complication following cataract extraction in patients with MD is transient iris rubeosis.15 Kuroda and associates reported on a patient who developed bilateral iris rubeosis postoperatively. Without treatment, the condition began to regress spontaneously two weeks after the cataract surgery.
Most commonly seen in ocular ischemic diseases, such as diabetic retinopathy, iris rubeosis develops near the pupillary border, and can lead to angle neovascularization and elevation of intraocular pressure. This patient did not experience the latter two conditions, and we observed him until resolution.
The iris rubeosis associated with MD is related to a defect in the blood-retinal barrier. The barrier is disrupted during surgery, resulting in leakage of chemical mediators and vascular endothelial growth factors.15 Following surgery, the blood-retinal barrier is able to restore itself, and spontaneous regression of the rubeosis is typical.15
Ptosis and extraocular muscle involvement are other common ocular manifestations of MD. Bilateral ptosis develops in approximately 80% of patients, and is due to weakness and atrophy of the levator muscle.1,2,4,11,17 The orbicularis oculi is also weakened, leading to lagophthalmos and infrequent blinking, which can result in exposure keratitis and dry eye symptoms.1,2,4,11 If ptosis repair is recommended, be careful to not over-correct the patient and make the eyelid closure worse.
Rarely, symptoms of diplopia and signs of gaze restriction will present. However, large amounts of exophoria are common, and often lead to convergence insufficiency.1,4,17 Mild reduction in saccadic velocity has also been reported.17-19
Low intraocular pressure results from decreased aqueous production caused by both atrophy and degeneration of the ciliary body.1 A patient with MD has an average intraocular pressure of 10mm Hg. Over time, this number decreases, resulting in readings of 8.5mm Hg in patients between the ages of 50 and 57.1,4 Macular changes are present in approximately 20% to 30% of patients with MD, and show a slow progression of streak-like, stellate or butterfly-shaped pigmentary changes in the retinal pigment epithelium.1,4,6,7
An accumulation of lipofuscin in the macular area of these patients has been reported; this correlates with muscle biopsies in MD patients also showing an increase in lipofuscin.6,11 Peripheral retinal findings may be seen in up to 50% of patients, and often consist of pigmentary clumping and atrophic changes.1,2,7 Routine monitoring of MD patients, including tonometry, Amsler grid assessment and dilated fundus examinations is necessary to observe any changes in ocular complications associated with the disease.
Differential diagnosis of MD includes myasthenia gravis, mechanical, traumatic or myogenic ptosis, chronic progressive external ophthalmoplegia, Kearns-Sayre syndrome and oculopharyngeal muscular dystrophy.1,11,20 Although ptosis and extraocular muscle weakness are commonly associated with many of these conditions, the characteristic polychromatic cataracts are unique to MD. Genetic testing, lab work, and muscle histology can also help make the appropriate diagnosis.
The diagnosis of MD is typically made clinically through a careful family history evaluation and both the physical and ocular examination. Laboratory tests may include testing the blood level for the muscle enzyme, creatine kinase.
Electromyography is another test that is used to examine the response of a muscle to stimulation. A small needle electrode is inserted, and the patient is asked to contract the muscle. The electromyograph analyzes the activity for any abnormalities, such as a decreased response that is seen in myotonic dystrophy.1
Muscle biopsies, though not routinely performed, show an irregular arrangement of myofibrils, disorganization of muscle fibers and an increase in lipofuscin.11 A truly definitive diagnosis can be obtained through DNA testing, which is used to confirm the genetic mutation in MD.
Currently, there is no cure for MD. Once diagnosed, management involves routine care aimed at preventing and treating the complications of the disease, including muscle weakness, and cardiac and respiratory complications. Both genetic counseling and patient education should also be considered. Given the risk of exposure keratitis secondary to the myogenic ptosis and lagophthalmos, take care to protect the cornea using lubrication, punctal plugs, lid taping, or even tarsorraphy.
Surgical management of the myogenic ptosis should be conservative, and should only be considered when the vision is compromised by lid position. Special care is necessary with any surgical procedure that requires general anesthesia, as the potential for respiratory complications and enhanced myotonia are present.1
Recommend cataract surgery when the lens opacities become visually significant. However, inform both the patient and surgeon about the potential postoperative complications, such as recurrent posterior capsular opacification and rubeosis irides.
We will likely consider referring our patient for cataract surgery in the next few years. His uncorrected visual acuity is already reduced to 20/40 O.U., secondary to his cataracts.
The future of MD management involves genetic research aimed at developing a method to reduce the CTG repeats on the DMPK gene.13 Much more data needs to be analyzed; however, new discoveries will likely provide more effective approaches to managing this disease.
1. Thomann KH, Marks ES, Adamczyk DT. Primary Eyecare in Systemic Disease. 2nd ed.
2. Steele BA. Ocular Manifestations of Systemic Disease: Making the Right Connections. Lecture and outline presented at the
3. Garrott HM, Walland MJ, ODay J. Recurrent posterior capsular opacification and capsulorhexis contracture after cataract surgery in myotonic dystrophy. Clin Experiment Ophthalmol Dec 2004;32(6):653-5.
4. Burian HM, Burns CA. Ocular changes in myotonic dystrophy Am J Ophthalmol Jan 1967;63(1):22-34.
5. Meola G, Moxley RT. Myotonic dystrophy type 2 and related myotonic disorders J Neurol Oct 2004;251(10):1173-82.
6. Sarks J, Liu H, Killingsworth M, et al. Retinal changes in myotonic dystrophy: a clinicomorphological study. Aust N Z J Ophthalmol Feb 1985;13(1):19-36.
7. Kimizuka Y, Kiyosawa M, Tamai M, Takase S. Retinal changes in myotonic dystrophy. Clinical and follow-up evaluation. Retina 1993;13(2):129-35.
8. Guimares AS, Carlsson GE, Marie SKN. Bite force and handgrip force in patients with molecular diagnosis of myotonic dystrophy. J Oral Rehabil Mar 2007;34(3):195-200.
9.
10. Gamez J. Bilateral optic nerve atrophy in myotonic dystrophy. Am J Ophthalmol Mar 2001;131(3):398-400.
11.
12. Turnpenny P, Clark C, Kelly K. Intelligence quotient profile in myotonic dystrophy, intergenerational deficit, and correlation with CTG amplification. J Med Genet Apr 1994;31(4):300-5.
13. Pizzuti A, Friedman DL, Caskey CT. The myotonic dystrophy gene. Arch Neurol Nov 1993;50(11):1173-9.
14. Traboulsi EI. Polychromasia capsulare (multicolored capsule): report of three families. Trans Am Ophthalmol Soc 2005;103:3-7.
15. Kuroda T, Katai N, Yoshida N, et al. Rubeosis iridis after bilateral cataract surgery and its spontaneous regression in a patient with myotonic dystrophy. J Cataract Refract Surg May 2006;32(5):873-4.
16. Gjertsen IK, Sandvig KU, Eide N, et al. Recurrence of secondary opacification and development of a dense posterior vitreous membrane in patients with myotonic dystrophy. J Cataract Refract Surg Jan 2003;29(1):213-6.
17. Yamashita T, Matsubara E, Nagano I, et al. Bilateral extraocular muscle atrophy in myotonic dystrophy type 1. Neurology Aug 2004;3(4):759-60.
18. Anastasopoulos D, Kimmig H, Mergner T, et al. Abnormalities of ocular motility in myotonic dystrophy. Brain Dec 1996;119(6):1923-32.
19. Versino M, Rossi B, Beltrami G, et al. Ocular motor myotonic phenomenon in myotonic dystrophy. J Neurol Neurosurg Psychiatry Feb 2002;72(2):236-40.
20. Abu-Baker A, Rouleau GA. Oculopharyngeal muscular dystrophy: recent advances in the understanding of the molecular pathogenic mechanisms and treatment strategies Biochim Biophys Acta Feb 2007;1772(2):173-85.
