The following case is featured in the "You Make The Diagnosis" section of the March 2024 Optometric Retina Society quarterly e-newsletter, which can be found here.
 |
| Click image to enlarge. |
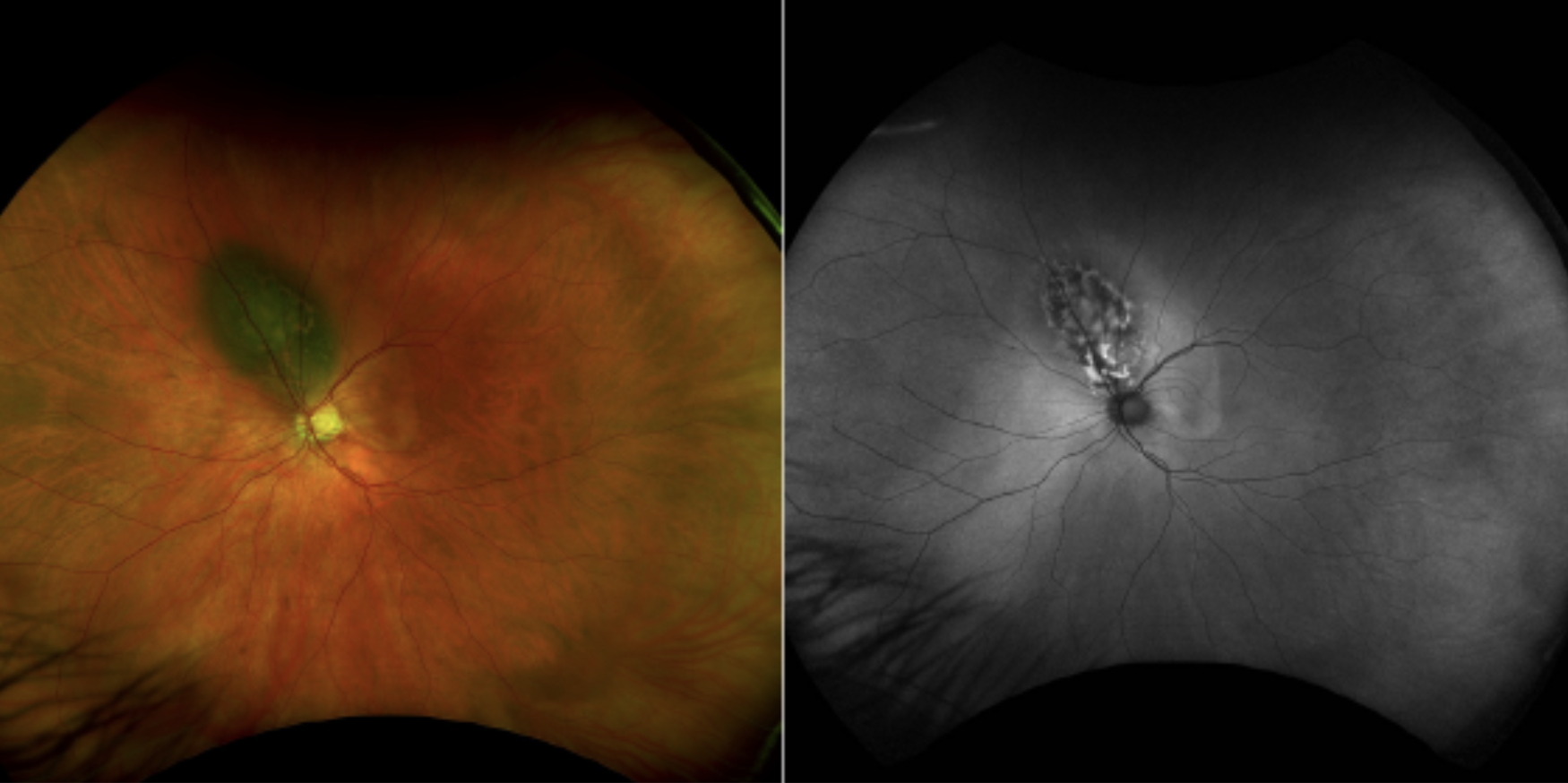
Choroidal melanoma is a tumor of the posterior uvea developing from melanocytes. It is the most common primary intraocular malignancy and second most common overall ocular malignancy following choroidal metastasis. The tumor can arise de novo, as seen in this case, or from malignant transformation of a choroidal nevus. Multimodal imaging technology is emphasized to distinguish choroidal melanoma from benign choroidal nevi. The imaging features most predictive of choroidal nevus transformation to melanoma include thickness >2 mm, subretinal fluid, orange pigmentation/lipofuscin, acoustic hollowness on ultrasound and largest basal diameter >5 mm on photography.1 For small choroidal lesions, thickness is most accurately measured on EDI SD-OCT and larger lesions on ultrasound.2 Subtle subretinal fluid is best detected utilizing OCT. Orange pigmentation corresponds to lipofuscin, a retinal byproduct indicating high metabolic activity, which is best appreciated with fundus autofluorescence. Independently, orange pigmentation imparts a 37% 5-year growth risk.1
Treatment of choroidal melanoma is dependent on clinical factors such as size, location and visual acuity. The most common treatment is radiotherapy, typically plaque brachytherapy and less often proton beam radiotherapy. Adjunctive treatments can be utilized such as transpupillary thermotherapy (TTT) or photocoagulation. The combination of plaque brachytherapy and TTT demonstrated only 3% tumor recurrence rate.3 Intravitreal anti-vascular endothelial growth factor can be employed to reduce the complication risks of radiotherapy, particularly radiation retinopathy. Enucleation of the eye is reserved for advanced melanoma or eyes that develop complications from radiotherapy. Tissue biopsy using fine needle aspiration can be performed to prior to plaque placement or after enucleation. These are sent for gene expression profiling which offers a risk profile for metastasis. Those with BAP1 genetic mutations have the highest 5-year risk for metastasis at 72%.4 The risk for metastasis also rises with increasing tumor thickness.5 The liver is the most common site for metastasis to occur.
| 1. Dalvin LA, Shields CL, Ancona-Lezama DA, et al. Combination of multimodal imaging features predictive of choroidal nevus transformation into melanoma. Br J Ophthalmol. 2019 Oct;103(10):1441-1447. 2. Shields CL, Kaliki S, Rojanaporn D, Ferenczy SR, Shields JA. Enhanced depth imaging optical coherence tomography of small choroidal melanoma: comparison with choroidal nevus. Arch Ophthalmol. 2012 Jul;130(7):850-6. 3. Shields CL, Cater J, Shields JA, et al. Combined plaque radiotherapy and transpupillary thermotherapy for choroidal melanoma in 270 consecutive patients. Arch Ophthalmol 2002; 120: 933–940. 4. Field MG, Harbour JW. Recent developments in prognostic and predictive testing in uveal melanoma. Curr Opin Ophthalmol. 2014 May;25(3):234-9. 5. Shields CL, Furuta M, Thangappan A, et al. Metastasis of uveal melanoma millimeter-by-millimeter in 8033 consecutive eyes. Arch Ophthalmol 2009;127:989–998. |