 |
A 73-year-old African female presented with a chief complaint of blurry vision OS>OD of two months’ duration. She was able to pinpoint that the persistent/constant blur developed after a sneeze. She denied trauma. Her previous ocular and systemic histories were remarkable for hypertension, for which she was properly medicated and compliant. She denied any known allergies to medications or other substances.
Clinical Findings
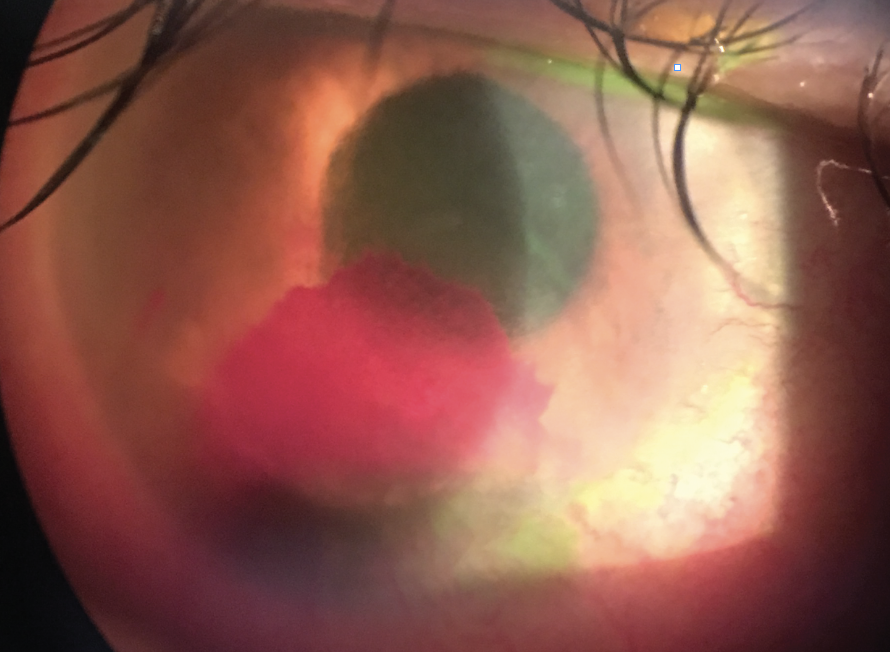
Her best-corrected entering visual acuity was 20/200 OD and 20/30 OS at distance and near. Refraction revealed hyperopia of +0.75 OD and +1.50 OS with no improvement in vision. The pertinent biomicroscopic findings are illustrated in the photograph.
Her intraocular pressure (IOP) readings measured as 35mm Hg OD and 18mm Hg OS using Goldmann applanation tonometry. Dilated fundus examination revealed no significant posterior pole or peripheral retina findings: the nerves were distinct with cup-to-disc ratios of 0.3/0.35 OD and OS.
For More Information
Additional studies included optical coherence tomography in each eye to examine the status of the nerve fiber layer and assess for evidence of glaucomatous damage, given the high IOP. An extensive dilated examination was completed to rule out the presence of mid-peripheral hemorrhages. Laboratory and Doppler testing was ordered to rule out the presence of other undiagnosed systemic diseases, such as diabetes and carotid artery disease. Gonioscopy was not completed so as not to increase the risk of rebleed; this could be completed at a later date.
 |
|
This was the patient’s presentation on slit lamp exam. She reported blurry vision as well. Click image to enlarge. |
Diagnosis
This is a case of hyphema secondary to ocular ischemic syndrome with secondary neovascular angle closure glaucoma in the setting of corneal blood staining.
Hyphema is defined as the presence of blood in the anterior chamber.1-4 Although the most common etiology is blunt trauma, a spontaneous hyphema may occur secondary to rubeosis iridis, xanthogranuloma, intraocular tumor, myotonic dystrophy, keratouveitis, iris vascular tufts or intraocular surgery.1,2 Presenting symptoms typically include dimming or changes in vision and sudden onset of floaters. Although the hemorrhage will typically resorb after a period of one to two weeks, careful management is required to avoid vision-threatening complications such as intraocular pressure (IOP) rise, corneal blood staining and risk of a rebleed.1
Pathophysiology
Iris neovascular blood vessels are prone to bleeding owing to their fragility and dynamic posture upon the iris. When they hemorrhage into the anterior chamber, the blood mixes with aqueous producing “micro” hyphema before settling inferiorly to form a layered hemorrhage.1,2 The sudden increase in volume within the anterior chamber rapidly increases the pressure inside it, permitting a self-tamponade. This assists blood clotting over the offending vessel.2 The trabecular meshwork (TM) is slowly unobstructed as the blood breaks down and resorbs over a period of weeks.1 Surgical evacuation of the anterior chamber is rarely indicated except in severe cases.2,4
Hyphemas can be graded by the percentage of the anterior chamber volume that is filled with blood (from the bottom to the top).1 Circulating blood cells in the anterior chamber without layering is termed “micro” hyphema. Grade 1 hyphema is defined as layered blood occupying less than one-third of the anterior chamber. Grade 2 hyphema is one-third to one-half of the anterior chamber occupied. Grade 3 is defined as more than one-half but less than the total anterior chamber occupied. Grade 4 (total hyphema) is when 100% of the visible anterior chamber is filled with blood. In some cases of grade 4 hyphema, circulation in the anterior chamber is impaired and the deoxygenated blood becomes dark in color. This can make the anterior chamber appear dark brown or black. This is the source for the term “eight-ball” hyphema.1
Acute elevation of IOP is at greater risk in proportion to the amount of layered blood in the anterior chamber. Secondary open angle glaucoma occurs in 10% of hyphema cases of grade 2 or less, 25% in grade 3 and 100% in grade 4 hyphema.1 The mechanism of the raised IOP is thought to be from direct obstruction of the trabecular meshwork by erythrocytes, fibrin, platelets and debris.1,3 Overall, this complication occurs in approximately 27% of patients with hyphema. The issue is usually self-limiting.3 There is a notable exception in the case of sickle cell disease patients who are prone to aggressive IOP response with even low grade hyphema.1,3 This is secondary to the increased propensity of the mis-shaped blood cells to occupy the drainage pathway, blocking aqueous egress.
The condition also increases the risk for optic neuropathy even in the setting of slightly abnormal IOP (>24mm Hg). Screening for sickle-cell disease should occur in all races where sickle cell anemia status has not been determined and the potential for undiagnosed disease exists.1
Another possible vector of increased IOP is pupillary block. Here, clotted blood completely covers the pupil.3
Corneal blood staining is a vision threatening complication of “micro” and large hyphemas. Prolonged contact with the corneal endothelium leads to deposition of hemosiderin on the endothelium with risk for penetration into the corneal stromal.5 Risk factors include the total size of the hyphema, prolonged contact with the affected area and elevated IOP.2,3,6 Overall incidence is 2% to 11%.1 When this occurs, hemosiderin typically deposits centrally and is slowly cleared peripherally in a centripetal fashion over two years’ time.1,5 Early surgical intervention is recommended in cases at high risk for blood staining, particularly in pediatric cases where amblyopia formation is possible.1
The occurrence of a rebleed is of concern as it typically worsens the severity from the original bleed and leaves the patient increasingly susceptible to visual loss from complications such as secondary open angle glaucoma and corneal blood staining.2 The incidence of rebleed is 6% to 33%1,3 and typically occurs between two and seven days after the initial injury.1,3 Rebleeding is primarily caused by retraction and or lysis of the fibrin-platelet clot over the ruptured vessel.1 The incidence of secondary glaucoma following rebleed is high at 45% to 67%.1 Risk factors for rebleed include race (African origin more common than Caucasian), sickle cell disease and initial size of the hyphema.1,2 Rebleed can be recognized clinically by an increase in size of the hyphema or observation of a fresh layer of blood over the older darker blood.1
Clinical Care
Management goals are focused on promotion of reabsorption of the hyphema and prevention of the above complications.1 Topical medical therapy in the form of cycloplegics (e.g.. atropine sulfate 1% QD-BID, homatropine 5 % QD-BID) and topical corticosteroids (e.g., prednisolone acetate 1% QID) are used to immobilize the iris, stabilize vascular permeability and resolve local inflammation.1,2 Elevated IOP can be controlled with topical aqueous-suppression medications in most instances. Beta-blockers and alpha agonists are preferred; prostaglandins and miotics are avoided to prevent any possible increase in vascular permeability along with aggravation of local inflammation.1,2,4 Oral agents such as acetazolamide or mannitol are used in cases where severe IOP elevation exists and cannot be reduced with topical agents alone.1 These preparations are contraindicated in cases involving sickle cell positive findings, as lowering of plasma pH can encourage sickling and its aforementioned complications. Methazolamide can be used as an emergent alternative.1
Reduced physical activity is a mainstay of management in all cases of hyphema.1,2 The patient should be instructed to sleep in the semi-Fowler position (sitting up, head elevated) and ambulate quietly until the hyphema resorbs. Hospital admission is necessary in some cases to allow for daily examination, pharmaceutical administration and close monitoring as well as direct enforcement of bed rest. Children, noncompliant patients, patients with severe hyphema or a predisposition to bleeding are all candidates for hospitalization.1,2 Use of an eye shield to reduce the possibility of recurrent trauma, especially during sleep, is also recommended until resolution is seen.1
Nasal decongestants and stool softeners may be used to eliminate Valsalva maneuvers. Oral analgesics with antiplatelet properties should be avoided. Temporary cessation of antiplatelet and anticoagulant therapy may be indicated in some cases and should be considered on a case by case basis in coordination with the patient's general physician.1
Oral antiplatelet therapy in the form of aminocaproic acid (ACA) is recommended in cases where there is a high concern for rebleed (except in cases with concurrent sickle cell disease where they are contraindicated).1 Oral corticosteroids can also be used for a similar benefit.1-3
Surgical intervention to prevent corneal blood staining or resolve an intractable IOP response can be performed in select cases where a lack of improvement is seen after one week.1,6 A layered hyphema that remains liquefied may be removed by limbal paracentesis and aspiration; however, the presence of a clot may require debulking with a vitrector.1
Daily follow-up of severe hyphema is necessary until a significant reduction in size is observed.1 Other patients should be seen one day after initial presentation and then again in one week. Once the hyphema has resolved and medical therapy is completed, the patient should be monitored every three to four months for IOP elevation that may occur secondary to the damage to the trabecular meshwork itself or by TM obstruction by ghost cells (de-hemoglobinized skeletons of red blood migrating forward from the anterior vitreous). Follow up may be subsequently lengthened as deemed appropriate by the clinician.1 Late glaucoma is possible for the remainder of the person’s life.
Gonioscopy should be performed following complete resolution of a hyphema to rule out angle damage, angle neovascularization or tumors requiring additional therapy, as well to determine if any peripheral anterior synechiae have formed.
If the underlying cause of the hyphema is not trauma, then its source must uncovered through laboratory or imaging investigations. Cases of hyphema from iris neovascularization must be treated both locally and systemically. Undiagnosed systemic disease must be identified and managed. The iris vessels may be regressed with combinations of panretinal photocoagulation and anti-VEGF. IOP control is classically difficult to achieve with medication alone. Trabeculectomy with antimetabolites or seton placement is often needed.7
Initial Management Plan
We initiated treatment with atropine 1% BID and prednisolone acetate 1% QID to control the inflammation and lowered the patient’s IOP using timolol 0.5%/brimonidine 0.2% BID and acetazolamide 500mg QD PO. We referred the patient to retinology to consider anti-VEGF injection to eliminate the neovascularization of the iris and angle and corresponded with her general practitioner to begin a systemic workup with testing and carotid artery imaging (B-scan).
Dr. Gurwood is a professor of clinical sciences at The Eye Institute of the Pennsylvania College of Optometry at Salus University. He is a co-chief of Primary Care Suite 3. He is attending medical staff in the department of ophthalmology at Albert Einstein Medical Center, Philadelphia. He has no financial interests to disclose.
1. Bansal S, Gunasekeran DV, Ang B, Lee J, Khandelwal R, Sullivan P, Agrawal R. Controversies in the pathophysiology and management of hyphema. j.survophthal.2015.11.005. Epub 2015 Nov 26. |
