 |
An incomplete medical and therapeutic history and the need to untangle often complex, vague past events to ensure the correct diagnosis can pose challenges to clinical care. In one particular case, a 59-year-old man was referred for evaluation of suspicion of glaucoma based on optic disc appearance. He reported taking three medications for Mycobacterium avium complex (MAC). While he wasn’t sure of the names of the medications, he did share that two drugs were oral tablets and the third was inhaled via a nebulizer. His vision was 20/20 in each eye, he had a subtle afferent pupillary defect in the right eye, intraocular pressure of 9mm Hg OD and OS, and superotemporal pallor of the right optic disc more than the left without notching of either neuroretinal rim. Deciphering his medical and treatment history through communication with managing providers led to the determination that he was taking rifampicin, isoniazid and inhaled liposome amikacin.
Background
Considered a mainstream illness in respiratory medicine, MAC pulmonary disease is a condition caused by non-tuberculosis mycobacteria.1,2,3 Unlike tuberculosis, the MAC group of pathogens are not contagious, but their increasing prevalence in the population and potential for serious ocular adverse events related to treatment mean that clinicians should be familiar with the condition and its management.4
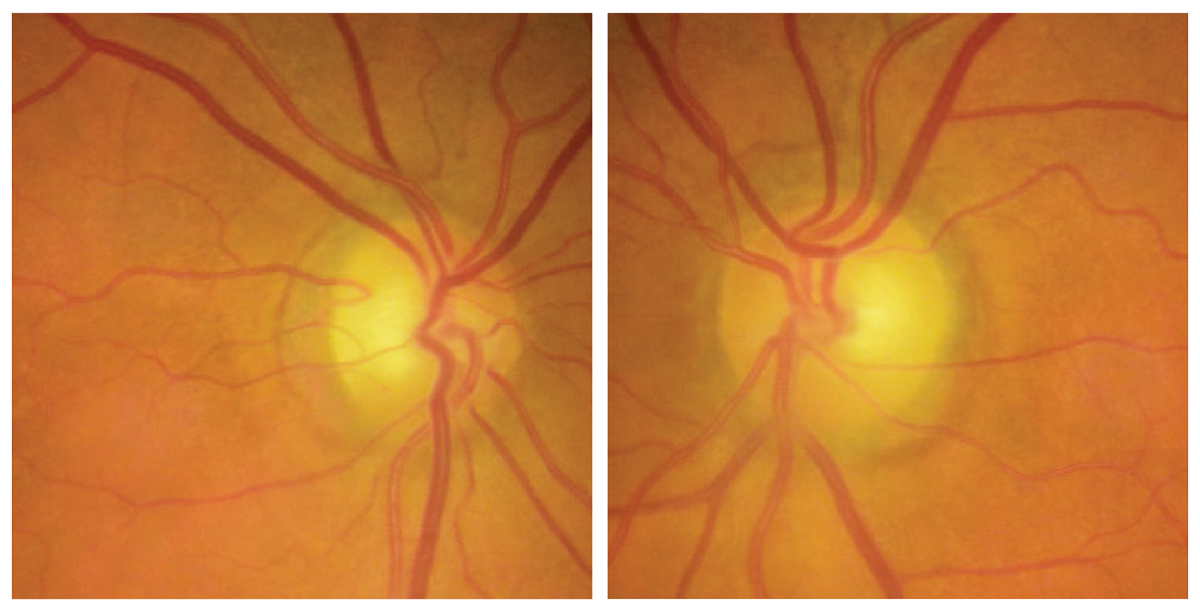 |
| Fig. 1. Optic disc photos demonstrating subtle superotemporal optic disc pallor of both eyes. Click image to enlarge. |
Mycobacterium avium, and the 11 other species of gram-positive, aerobic bacteria that are responsible for MAC pulmonary disease are generally not pathogenic and are naturally found in water and soil sources around the world.2,3 In susceptible immunocompetent individuals, which primarily include those with underlying pulmonary disease and those with past smoking history and bronchiectasis, widening and scarring of the airways result in the inability to clear mucus and MAC-causing bacteria after inhalation or ingestion resulting in infection that leads to symptoms of fatigue, shortness of breath and chronic cough.3
While diagnosis of MAC is made by clinical, radiologic and microbiologic evaluation, treatment is not always necessary in immunocompetent individuals.1,3 Careful evaluation of pathogenicity and individualized evaluation of risks and benefits of therapy may lead to the decision to monitor without antibiotic treatment. Even with aggressive long-term, multidrug therapy, clearance of the infection is not always possible, as a recent meta-analysis described the resolution rate of MAC in 3,800 individuals to be only 68.1%.5
Despite the lack of risk of contagious spread of MAC, when treatment is indicated, patients will generally be managed by an infectious disease specialist. Long-term antibiotic therapy for 18 or more months may be needed, with current guidelines recommending continued treatment for 12 months following conversion to negative culture.1 Standard therapy for MAC is a three-antibiotic regimen incorporating a macrolide (usually azithromycin), ethambutol and a rifampicin-based drug.1 The array of antibiotics used in MAC treatment are associated with known adverse systemic and ocular events that clinicians must be familiar with in order for prompt recognition and communication with the managing physician in order to minimize vision or life-threatening effects.
Incorporating ethambutol into the MAC treatment regimen, generally at a dosage of 15mg/kg/day, is primarily to prevent the development of Mycobacterium resistance to the prescribed macrolide and is considered a central component of therapy, even more so than for tuberculosis treatment due to the extended period of antibiotic therapy required.1,6,7 Patients have up to a 6% risk of ethambutol-associated optic neuropathy in MAC lung disease treatment regardless of the dosage, despite the risk generally being described as dose-related.8 While time to onset of ethambutol-associated optic neuropathy varies, a recent analysis identified that most patients experienced symptomatic change between 181 and 300 days after initiation of therapy.9
Monitor Treatment
Careful, frequent, ophthalmic evaluation that incorporates automated visual fields and retinal nerve fiber layer (RNFL) and ganglion cell analysis in individuals taking ethambutol have been recommended due to the risk of progressive, often irreversible vision loss and the goal of early diagnosis and intervention. For patients taking an ethambutol dosage greater than 15mg/kg/day, for those treated for longer than two months, and for those with renal insufficiency, monthly evaluation with visual symptom screening, visual acuity assessment and color vision evaluation have been recommended.10,11 Incorporation of automated visual field testing and RNFL and ganglion cell complex analysis in addition to clinical examination are advised for detection of asymptomatic, preclinical optic neuropathy. A recent prospective study of individuals taking ethambutol for tuberculosis for a period of six months identified that 46% of eyes demonstrated subclinical, asymptomatic change from baseline attributable to ethambutol toxicity detected by RNFL and ganglion-cell inner plexiform layer loss.12 Other agents that may be used in the treatment of MAC also have known ocular effects. Isoniazid, while a less common cause of optic neuropathy than ethambutol, has been reported to cause optic neuritis, and rifampin may cause the discoloration of tears, sweat, and saliva.13,14
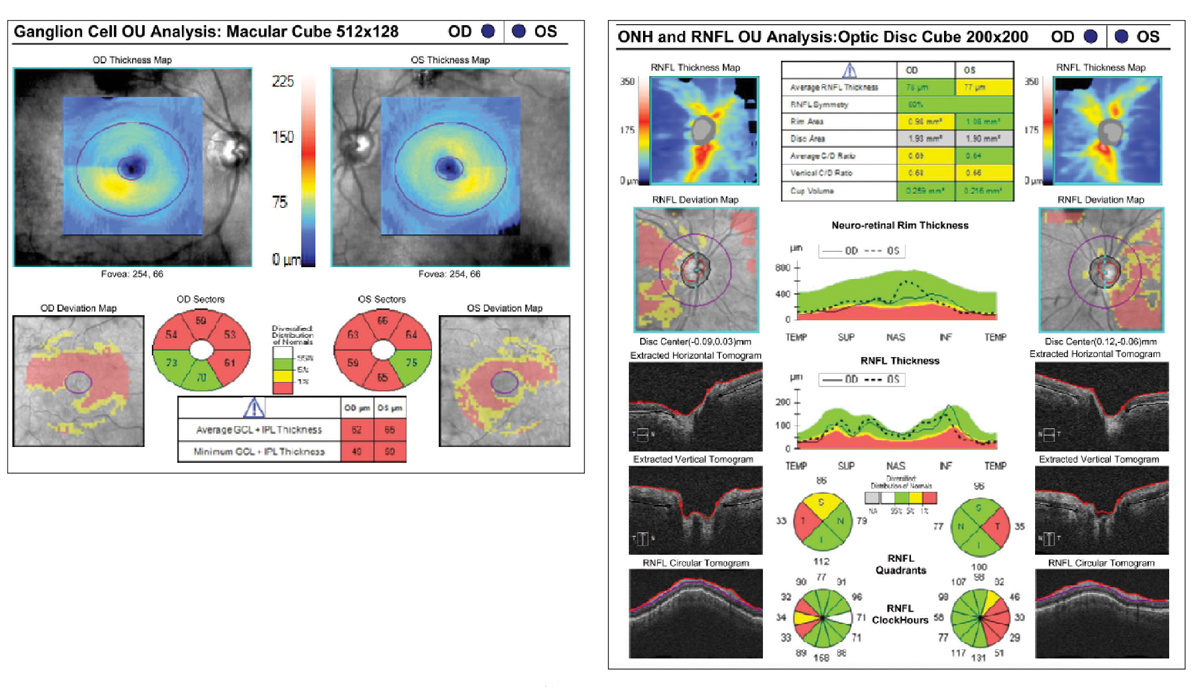 |
|
Fig. 2. Ganglion cell inner plexiform layer (left) and RNFL analysis (right) should be performed regularly on patients with MAC infection. Click image to enlarge. |
Unlike tuberculosis, MAC is not a reportable disease, which means that epidemiological data are uncommon. However, we do know that in North America, MAC prevalence is on the rise, primarily in older individuals, with a recent Canadian study identifying a 2.5-fold increase in the number of individuals diagnosed with MAC between 2010 and 2020.4 Proposed reasons for increased prevalence related to increased environmental exposure, the long duration of treatment and the rise of biologic agents resulting in low-grade immunosuppression.3,15
While standard therapy in MAC pulmonary disease relies on agents developed more than 30 years ago, advancements in MAC are continuing to be developed to meet the needs of patients and managing physicians. For individuals with MAC refractory to treatment after six months of standard therapy, the addition of the FDA-approved inhaled amikacin liposome suspension, Arikayce (Insmed), is recommended.1 While systemically administered aminoglycosides carry the risk of ototoxicity and nephrotoxicity, the risk of systemic exposure been proposed to be reduced with localized drug delivery to the lungs. In an open-label extension trial investigating the safety and efficacy of amikacin liposome suspension through an additional 12 months of treatment, 7.8% of participants experienced hearing loss and 6.7% experienced tinnitus with an additional 33.3% of treated individuals demonstrating culture conversion through 12 months.16
Patient Follow-up
Considering the patient’s clinical appearance of subtle optic atrophy in the absence of glaucomatous optic neuropathy, targeted questioning about MAC treatment history revealed the patient had been diagnosed with MAC in 2019, and after initial treatment of ethambutol, it was discontinued after approximately 22 months due to concern of ocular toxicity, with documentation of the absence of progressive optic neuropathy since the drug’s discontinuation. After nearly four years of continued antibiotic therapy for MAC, the patient continues to require ongoing multidrug treatment without conversion to negative culture. His current treatment regimen, while not including ethambutol, still requires careful clinical evaluation, periodic OCT of the RNFL and ganglion cell inner plexiform layer, as well as automated visual fields, due to known risk of ocular adverse effects and continued communication with his managing providers.
MAC pulmonary disease represents a heavy ailment and treatment burden on patients and their caregivers due to chronic morbidity and burden of long-term therapy with significant risk of toxicity, often without disease resolution. Recognizing the adverse ocular effects of systemic medications begins with an accurate and complete history, which often requires a great deal of legwork, as well as an up-to-date medical knowledge of the underlying disease process and potential ocular complications.
Dr. Steen is an associate professor at Nova Southeastern University College of Optometry where she serves as director of the Glaucoma Service, coordinator of the Primary Care with Emphasis in Ocular Disease Residency and teaches courses in glaucoma and ocular pharmacology. Her financial disclosures include Bausch & Lomb, Santen, Ocuphire and Carl Zeiss Meditec.
1. Daley CL, Iaccarino JM, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Clin Infect Dis. 2020;71(4):e1-36. 2. van Ingen J, Turenne CY, Tortoli E, et al. A definition of the Mycobacterium avium complex for taxonomical and clinical purposes, a review. Int J Syst Evol Microbiol. 2018; 68(11):3666–77. 3. Griffith DE, Aksamit T, Brown-Elliott BA, et al.; ATS Mycobacterial Diseases Subcommittee; American Thoracic Society; Infectious Disease Society of America. Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416. 4. Marras TK, Nelson P, Peci A, et al. Pulmonary nontuberculous mycobacteria, Ontario, Canada, 2020. Emerg Infect Dis. 2023;29(7):1415-9. 5. Nasiri MJ, Ebrahimi G, Arefzadeh S, et al. Antibiotic therapy success rate in pulmonary Mycobacterium avium complex: a systematic review and meta-analysis. Expert Rev Anti Infect Ther. 2020;18(3):263-273. 6. Morimoto K, Namkoong H, Hasegawa N, et al. Nontuberculous Mycobacteriosis Japan Research Consortium. Macrolide-resistant MAC lung disease: analysis of 102 consecutive cases. Ann Am Thorac Soc. 2016;13(11):1904-11. 7. Jarand J, Davis JP, Cowie RL, et al. Long-term follow-up of Mycobacterium avium complex lung disease in patients treated with regimens including clofazimine and/or rifampin. Chest. 2016;149(5):1285-93. 8. Griffith DE, Brown-Elliott BA, Shepherd S, et al. Ethambutol ocular toxicity in treatment regimens for Mycobacterium avium complex lung disease. Am J Respir Crit Care Med. 2005;172(2):250-3. 9. Ozawa T, Namkoong H, Takaya R, et al. Analysis of adverse drug events in pulmonary Mycobacterium avium complex disease using spontaneous reporting system. BMC Infect Dis. 2022;22(1):580. 10. MacVinish S, McMaster D., Moledina T, et al. Ethambutol and visual assessment in England: current practice and recommendations. Eye. June 22, 2023. [Epub ahead of print]. 11. Saxena R, Singh D, Phuljhele S, Kalaiselvan V, et al. Ethambutol toxicity: expert panel consensus for the primary prevention, diagnosis and management of ethambutol-induced optic neuropathy. Indian J Ophthalmol. 2021;69(12):3734-9. 12. Mandal S, Saxena R, Dhiman R, et al. Prospective study to evaluate incidence and indicators for early detection of ethambutol toxicity. Br J Ophthalmol. 2021;105(7):1024-8. 13. Kass I, Mandel W, Cohen H, et al. Isoniazid as a cause of optic neuritis and atrophy. JAMA. 1957;164(16):1740-3. 14. Snider DE, Farer LS. Rifampin and red urine. JAMA. 1977;238(15):1628.3. 15. Calabrese C, Winthrop KL. Mycobacterial infections potentiated by biologics. Infect Dis Clin North Am. 2020;34(2):413-23. 16. Winthrop KL, Flume PA, Thomson R, et al. Amikacin liposome inhalation suspension for Mycobacterium avium complex lung disease: a 12-month open-label extension clinical trial. Ann Am Thorac Soc. 2021;18(7):1147-57. |
