 |
We all have a tendency to slip into bad habits, especially as we aim for greater efficiency in our clinical exams. One test that some practitioners may overlook or omit in order to decrease chair time is stereopsis. Many practitioners perform stereo testing on new, younger patients but not established or adult patients in the belief that stereopsis does not change over time or that it is only needed in childhood. As we have observed, however, not only can stereo change, but regular assessment of stereo can provide insight into patients’ overall comfort and binocular stability. Here, we offer you a review of four commonly used stereo tests and discuss their clinical usefulness.
Functional Binocular Assessment Test (FBAT)
The FBAT (Bernell) is the new version of the older Keystone Basic Binocular Test (KBB) (Figure 1). Designed as a user-friendly flipbook, the FBAT is a red/green test that assesses all three levels of fusion: simultaneous perception (primary fusion), flat (secondary) fusion and stereopsis (tertiary fusion). With directions for each page written on the back of the next, the FBAT is easy to administer and requires only red/green glasses as additional equipment. While the test is typically used for toddler and preschool ages, we have used it on much younger patients by holding the red/green glasses ourselves and watching for a reaching reaction to perceived float of the targets. Even older infants will instinctively reach for engaging targets; the youngest patient who gave either of us a reaching response, attempting to grasp the hippo target and delighting her parents, was just four months old!
 |
|
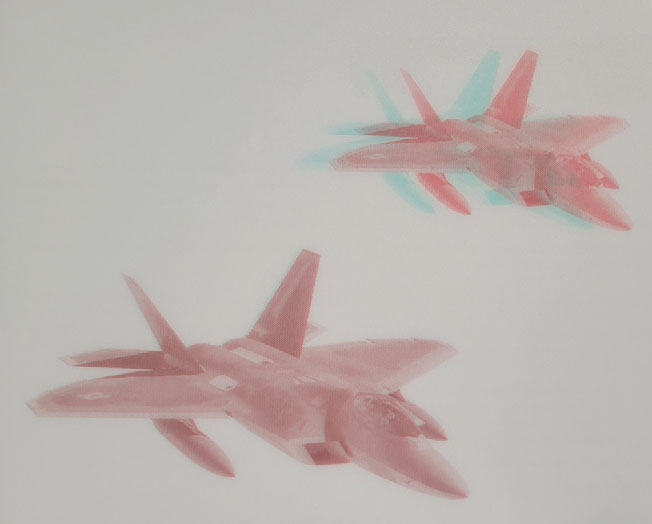
Fig. 1. FBAT jets showing local stereopsis demand. Click image to enlarge. |
A few particularly useful features exist on the FBAT. One is that several of the targets include a black circle around the red/green images. This circle is viewed by both eyes through the filters, providing a binocular fusion lock that can help patients perceive the appropriate stereopsis by stabilizing alignment. Stable visual axes make stereo easier to achieve and maintain. Another helpful feature is that some pages include multiple targets of different retinal disparities (and therefore different levels of stereo), allowing the practitioner to assess the patient’s flexibility. If they can jump quickly between targets and appreciate the appropriate depth, their vergence system is likely to be quite flexible indeed. A third clinically helpful feature is that at least one of the multiple-target pages includes images that are counterintuitive in their respective sizes.
For example, we see two jet planes in Figure 1. Looking at the targets without the red/green glasses, it is easy to see there is greater disparity in the smaller of the two planes; when seen in stereo, this plane should float closer to the patient than the larger plane. Patients who suppress an eye’s input and use monocular cues for depth, however, will report upon questioning that the larger of the two planes appears closer, since larger objects take up more retinal area, and we learn very early in life that this means “closer.” We can easily tell whether a patient is suppressing if they give this response.
Lang II
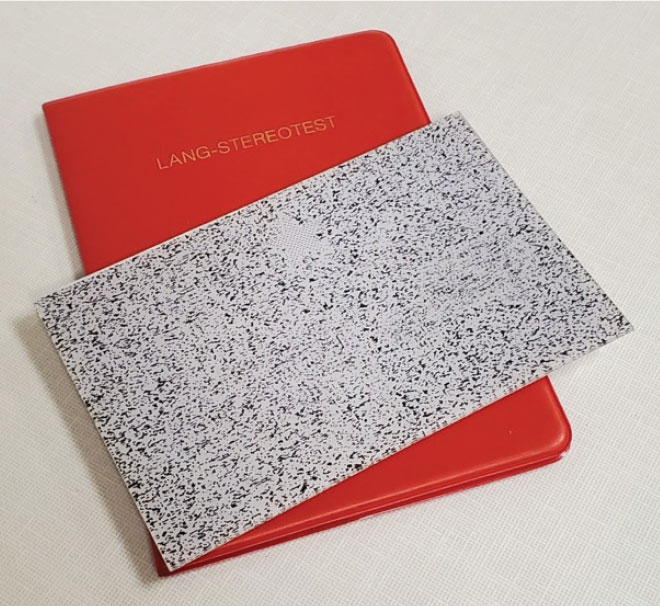
One difficulty that we occasionally face with younger patients is getting them to leave red/green or polarized glasses on for testing. The Lang Stereo Test (Bernell) is an option that does not require the use of glasses. It comes in two forms: Lang I and Lang II, which have targets of different stereo demand. I (PS) have carried a Lang II card with me for most of my 20+ years in practice and greatly appreciate its ease of use for youngsters.
The Lang II card (Figure 2) presents one demonstration and three global stereo targets; these are all in the form of kid-friendly pictures. Included in the test are a star (demonstration only, seen monocularly), a car, an elephant and a moon. These targets range from 600 arcseconds (the elephant) to 200 arcseconds (the moon) of base-out demand. However, they are difficult to see if the patient isn’t looking at them straight-on. This can lead to some interesting comments from parents, like, “Wow, I can’t see that!”—it’s a great way to suggest that they also schedule an exam.
 |
|
Fig. 2. The Lang II stereo test. Click image to enlarge. |
There are two types of stereo: global and local. Local targets have distinct edges or borders; the Wirt circles in the standard Randot book are good examples. In contrast, global targets do not have distinct borders and instead are random-dot presentations. For those part of Generation X (like me) and Baby Boomers out there, these are the ones that look like the old TV “snow” patterns! Using global targets to test stereopsis requires the patient to use both foveae in order to see them. Because of this, global targets are especially useful for strabismus patients, as we can immediately tell whether or not a turn is constant or intermittent. If the patient achieves global stereo, they are aligned and using both foveae—at least for that moment.
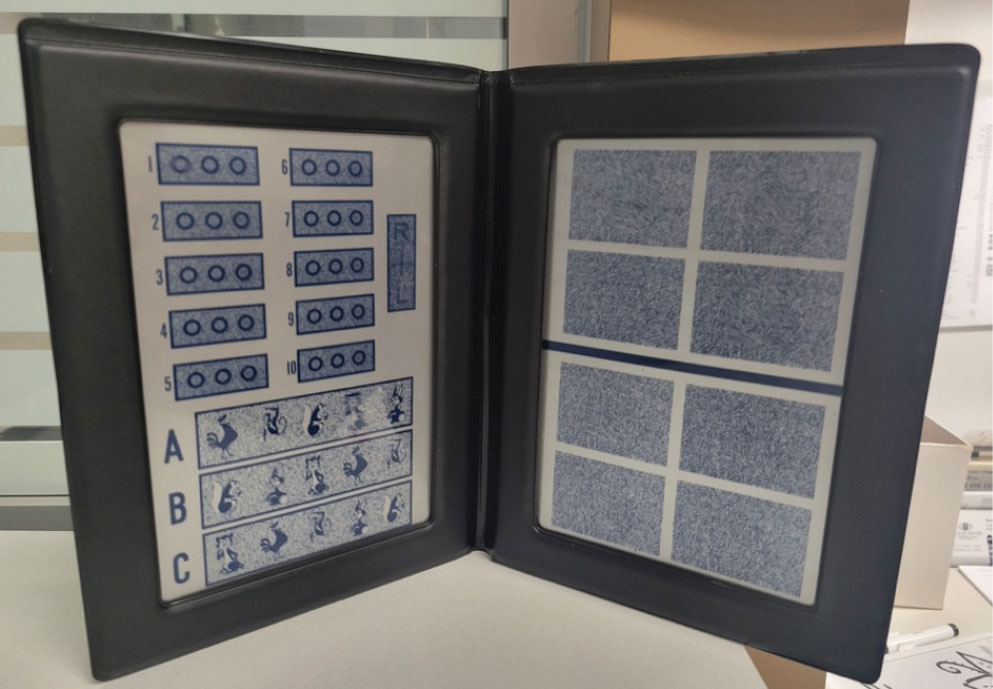
Randot
This is the classic book that most of us acquired and used during our optometry training (Figure 3). Using polarized glasses, patients are presented with both local and global stereo targets that cover a wide range of demand. On one page, there are Wirt circles, arranged either in groups of three or four, depending on the specific book you have. Local stereo demand can be as small as 20 arcseconds for these targets, providing a very precise assessment of stereo acuity. Since patients may give up when the targets become difficult to discern, it’s important to encourage them to keep guessing—they often are able to visualize depth in much finer increments than they realize.
 |
|
Fig. 3. The Randot stereo test, showing both local and global targets. Click image to enlarge. |
One observation I have made over the years is that fine stereo often decreases prior to noticeable drops in visual acuity, so I find it helpful to test using Wirt circles every year and look closely for changes. The circles can also be used to determine immediate change with nearpoint prescriptions.
The other page of the Randot (Stereo Optical) book displays a series of shapes or forms, presented as global targets. Patients are asked to point out and to identify the shapes seen in the boxes; most books include four boxes on the top of the page with a 500 arcsecond demand and four boxes on the bottom with a 250 arcsecond demand. There is usually one “empty” box in each group of four that contains no discernible shape, which provides a check on whether patients are making up answers. For young patients who may not yet know the names of the various shapes, I find it useful to flip the book closed and have them match the shapes printed on the cover.
Bernell Evaluation of Stereo Test (BEST)
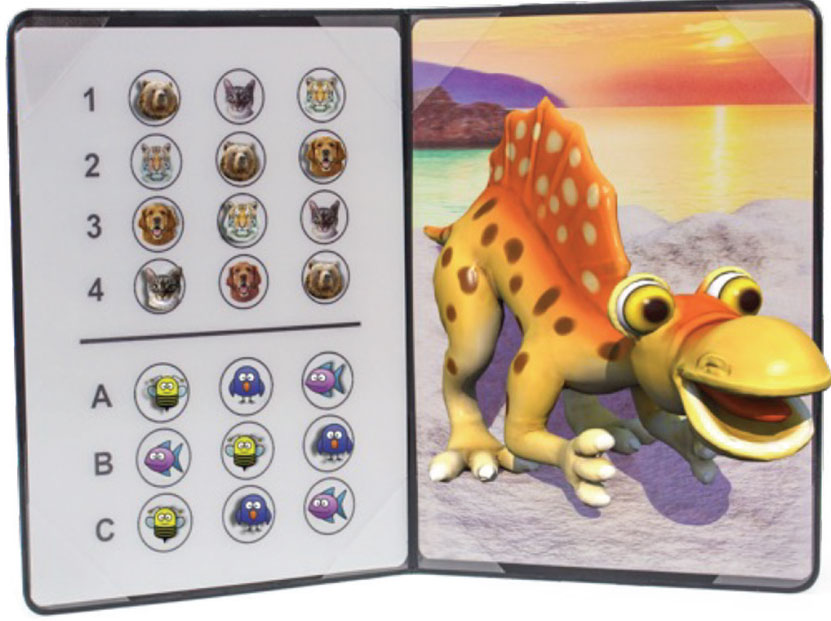
This newer stereo option is an especially kid-friendly test since it uses cartoon-style characters (Figure 4). All the targets on the BEST are local stereopsis, created with lenticular technology that does not require glasses to produce the stereo effect. Additionally, it is the only test reviewed of the four here that is in color, which can better help in keeping kids’ attention on the task.
On one page of the BEST, pictures of different animals are arranged in multiple rows of three. One animal in each row is neutral, one animal is a base-in target and one animal is a base-out target. Stereo demand on the top set (numbered one to four) ranges from 400 to 40 arcseconds; demand on the targets below (lettered A to C) goes down to 80 arcseconds. On the facing page, a large, friendly dinosaur greets patients with its head down and a big smile—no teeth! The stereo demand varies across this target, and most of my young patients giggle while trying to “catch” the dino’s nose, ears, toes, etc. I find it a fun way to check stereo in the preschool population in particular.
 |
|
Fig. 4. BEST stereo test, dinosaur. Photo: Bernell Corporation. Click image to enlarge. |
Takeaways
Although it may seem to be just another step in the exam sequence, one that takes time and may slow down clinical flow, stereo testing is actually fairly quick to perform and can provide important information, ranging from slight changes in visual status to differentiation between intermittent and constant strabismus. It can be easily taught to paraoptometric technicians, making its incorporation into your practice even more seamless. We recommend adding stereo back into your sequence—or continuing to include it!
Dr. Taub is a professor and co-supervisor of the Vision Therapy and Pediatrics residency at Southern College of Optometry (SCO) in Memphis. He specializes in vision therapy, pediatrics and brain injury. Dr. Schnell is a professor at SCO and teaches courses on ocular motility and vision therapy. She works in the pediatric and vision therapy clinics and is co-supervisor of the Vision Therapy and Pediatrics residency. Her clinical interests include infant and toddler eye care, vision therapy, visual development and the treatment and management of special populations. They have no financial interests to disclose.
