Vision CareCheck out the other feature articles in this month's issue: - Kids and Screens: Debating the Dangers |
The success story of optometry over the last few decades can be attributed in part to our early embrace of medical eye care, first and foremost as a service to society—filling a void created as an aging population strains the capacity of a stagnant ophthalmology infrastructure—but also as a means of diversifying our revenue base and challenging our minds with the complexities of disease diagnosis and treatment. Today, optical, medical and surgical care (largely through comanagement) are all within our ambit.
Optometry, in this new guise, is flourishing. And it’s a good thing too, because the optical component that was our lifeblood for a century has been steadily declining and shows no sign of reversing its course. Where we once were the gatekeepers of vision care, nowadays we’re merely a part—albeit a big one with enormous public goodwill—of a somewhat chaotic and complex distribution system. The once-simple process of getting a pair of glasses is now a morass of competing and not-always-cooperating entities: vision plans, insurance carriers, dedicated optical shops, optometric chain stores, medical eye care practices, direct-to-consumer retailers of corrective lenses and, lately, the anticipated rise of online refraction services. Let’s review how some long-time practitioners are faring in this volatile environment and what strategies for success can be gleaned from their experiences in the trenches.
Pump Up the Volume
Anyone who has been involved in optometry for any length of time can tell you the ways “things have changed since they first started.” The year 2020 alone, thanks to COVID, has shaken up the profession and made us rethink the way we clean things, see patients and do business. It was a tough year that often left us struggling to find new strategies on how to adapt. Then again, optometry is an ever-changing profession and has been learning to adapt to the challenges of the day for virtually its entire existence.
Jeffrey Roth, OD, together with his father, Michael S. Roth, OD, have collectively witnessed how the profession has changed over the last five decades. The elder Dr. Roth opened cold in 1973 and built a practice from the ground up in Syracuse, NY. After 30 years of hard work, he sold the practice to his son once he decided to move to California to semi-retire.
Even back in Dr. Michael Roth’s day, opening cold was anything but easy. “He once told me a story about how he had two patients—as in, only two patients in the entire practice,” Dr. Jeffrey Roth says. “One day, one [of the patients] walked in wanting him to adjust their glasses. He sprung up, whirled the glasses around in his hands and managed to snap them into two pieces. I quickly asked him, ‘What did you do then?’ He just calmly replied, ‘Well, then I had one patient.’”
Dr. Roth admits a lot has changed since his dad started practicing. Dealing with declining insurance reimbursements, online sales of glasses and contacts and “big-box” competitors have been some of the challenges Dr. Roth finds himself up against today as a private practice owner. “Optometry has always had its challenges. My father’s was an all-cash business—full retail payment for glasses and contacts—[but now], insurances have made things a nickel-and-dime discussion. I’m sure some people don’t even walk through the door if we don’t take their insurance.”
With reimbursements dropping every year and costs always on the rise, Dr. Roth, like thousands of other ODs, has had to drop a few insurance plans—and carefully manage the disengagement from care of long-time patients. “Heck, I saw one family over two years and didn’t get paid for a single claim. I was working for free. I just couldn’t take that plan anymore,” Dr. Roth says.
Optometric practices have been able to survive the continual decline in third-party reimbursements so long as patient volume was steady or growing. Pandemic-related shutdowns last year showed just how dependent many practices are on patient volume—and the ensuing dispensary revenue—when it abruptly dried up in mid-March. A recent report from the Vision Council notes that independent eye care providers experienced a 13.2% decline in optical sales from September 2019 to September 2020. Weekly sales and revenue data from Jobson Research shows how all measures of an optical’s performance remained depressed from late-March to the end of 2020 (Figure 1).
Perhaps the COVID crisis will push more ODs to finally opt out of their worst plans. However, there are ODs out there like Michael B. Silverman, OD, who opened his practice in Coral Springs, FL, cold in 1996. He says that, unlike Dr. Roth, he doesn’t plan on dropping any vision plans despite their reimbursement rates plummeting over the years. He has, however, started focusing on making his office run as efficiently as possible and added new technologies that help him do so in order to see a higher volume of patients to compensate for the lower payments he’s receiving.
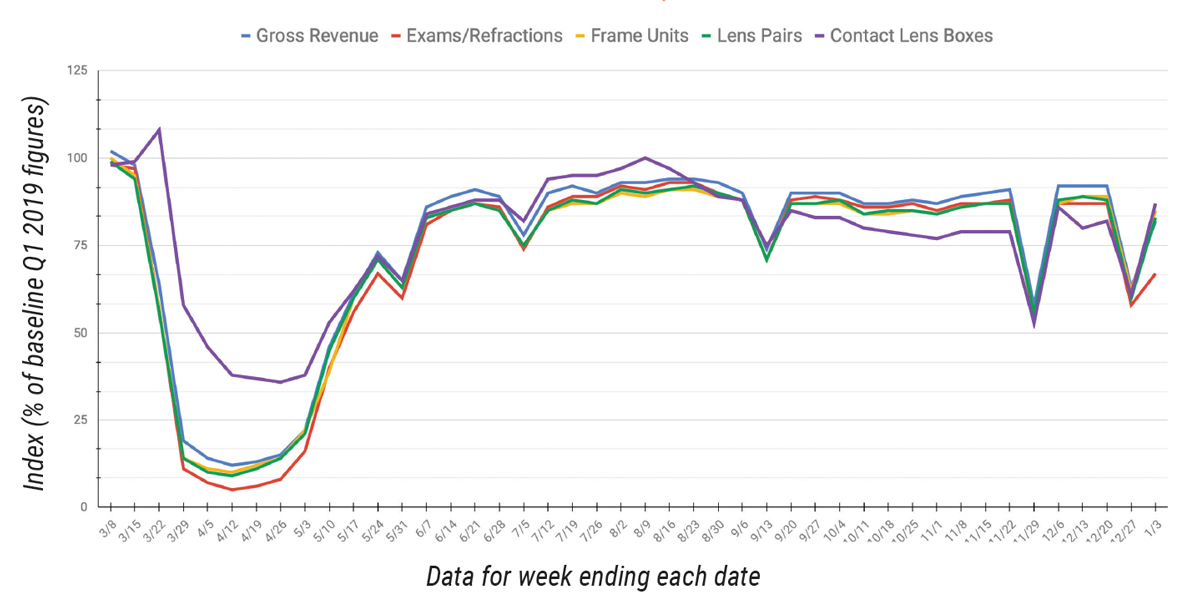 |
The index baseline, represented by a figure of 100, was developed from an average of seven days in the first quarter of 2019. All other time periods are calculated as a percent increase or decrease from the 100 baseline index of that period. Source: Jobson Research. Click image to enlarge. |
“Vision plans are a ‘two-edged sword,’” Dr. Silverman says. “On the positive side, they can generate a huge number of new patients and customers, especially for a new practice.” Keep those patients happy and they’ll refer co-workers, friends and family your way. “On the negative side, the reimbursements for eye exams and glasses through these vision plans are dismal and require you to see more patients per day to keep up revenue.” Unfortunately, he adds, “Despite how much patients appreciate me and my services, they will go elsewhere if I no longer accept their vision plan.”
Product sales margins are also continually being squeezed. Dr. Roth says, “We need industry to give us a fighting chance when it comes to the optical side of things, be it with cost of goods or access to inventory.” Dr. Roth also laments the consolidation of industry power through mergers and acquisitions. “We should look for ways to bring in fair market competition.”
In a bitter irony, practices feel the heat of competition from big-box retailers but have no recourse to level the playing field, especially in contact lens sales. The new FTC rule on contact lens release saddles optometrists with onerous new paperwork hassles to document prescription release and looks the other way at the transgressions of online lens retailers, like product substitution and passive verification.
Dr. Roth says he is trying not to worry about online retailers and hopes that patients will recognize the skill and hard work that goes into his practice to deliver a high level of quality care. “Online entities do not have any interest in the health and well-being of the patient, so I don’t try to compete with them. I educate my patients regarding their health and show [them] how I can make a difference.” He also says that while online retailers have made the sales of glasses and contact lenses harder, “Price-wise, I can’t compete, and if I tried to, it would be a race to the bottom, so that’s not something I’m willing to do.”
Dr. Silverman postulates, “For the next few years, from a business point of view, the biggest obstacles and challenges for private practice ODs and those with retail optical shops alike will undoubtedly be the presence of online retailers selling glasses and contact lenses and giving online eye exams.” Dr. Silverman says, “Profits from glasses and contact lens sales will continue to drop off significantly due to this mass swing for buying products online.”
However, he thinks that online eye exams themselves will not take as big of a bite out of the market as some might fear, and he adds that he has already seen inaccuracies and misdiagnoses with online exams. To reassure us, he says, “There will always be people who appreciate direct, person-to-person care. The optometric community has to continue reaching our high standards and show the public that our world-class, in-person eye care services are far superior to [those of] online eye exams and services.”
Time for Telehealth?The issues Drs. Roth and Silverman relate are not the only obstacles optometry has been working to overcome in recent years, and it seems there will be even more changes in the future. “Optometry will face many challenges and opportunities as we navigate the next decade together,” says Howard Purcell, OD, president and CEO of the New England College of Optometry. “Dealing with the pace of change will be the primary issue—that in itself brings both challenge and opportunity.” Dr. Purcell notes that artificial intelligence, virtual reality, telehealth and 3D printing are a few important examples of disruptive technology. He’s of the opinion that these trends, when properly harnessed, can bring a new source of financial support to optometric practices. Dr. Purcell encourages ODs to meet these changes and the pace of change head-on. “We must embrace, critique, validate and test these new technologies and identify their true value. Encouraging more innovation from within the profession will be essential,” says Dr. Purcell. Telehealth is one such innovation that Dr. Purcell urges ODs to consider adopting, especially as the pandemic has already demonstrated its potential value. “Telehealth and its associated opportunities are here and now. It is a great adjunct to our care delivery when used appropriately.” Of course, most practices learned this the hard way during last year’s practice shutdowns, as telehealth was the only means most of us had of extending any sort of care to our patients. Dr. Purcell encourages ODs to stick with it and find ways to integrate these capabilities on a regular basis, even after the pandemic. “Telehealth can be an important vehicle to, for example, triage emergencies, manage contact lens follow-ups, lead vision therapy sessions and facilitate at-home low vision device evaluations.” He also points out one often-overlooked component of telehealth: the opportunity for doctor-to-doctor consultations of cases, which can improve patient outcomes and satisfaction. “I would recommend all ODs critically evaluate these new technologies and maintain an open mind to the opportunities and advantages they may ultimately provide.” In March 2020, the American Optometric Association (AOA) held a free webinar on telehealth and telemedicine to help teach ODs about the different types of telehealth and how to bill and code for each. AOA members can find more information on telehealth and how to incorporate it into practice on the organization’s website under the “Guide to Telehealth-Based Care” section. |
Vision Correction Evolves
Of course, it’s not enough just to get patients through the door; they also need to be motivated to purchase corrective lenses from you. Here, optometric practices face pressures most notably from online sellers but also perhaps from newer optical corrections with enough long-term success that they might reduce or eliminate recurring product sales.
Some ODs have pondered, similar to the trepidation they experienced with the development of refractive surgery decades ago, whether the array of premium IOLs (multifocal, toric and multifocal toric) could work so well that they might cause a decline in revenue for the optical dispensary side of practices. The short answer: not yet, but better designs are continually pushing the envelope.
Eric Donnenfeld, MD, a founding partner of Ophthalmic Consultants of Long Island and clinical professor of ophthalmology at New York University, says optometrists should not fret but rather focus on how to better build their comanagement relationships with MDs. He says his cataract practice has grown dramatically over the last several years as the population ages and interest in quality surgical outcomes grows. “Concomitantly, as technology has improved, so has my use of premium IOLs,” he says. “Currently, I implant 20% multifocal IOLs, 15% toric IOLs and 5% multifocal toric IOLs.”
“There is no doubt that multifocal IOL technology continues to improve,” says Dr. Donnenfeld. “The most recent generation of IOLs has much better vision quality at distance while providing near vision as well. However, the use of presbyopic IOLs has not grown significantly over the past decade and remains at a 6% market share of all cataract surgeries.” He explains that the newest generation of presbyopic IOLs, Vivity (Alcon) and Eyhance (Johnson & Johnson Vision), are refractive rather than diffractive and do not split light. “They provide better distance vision than previous generations of multifocal IOLs but only intermediate vision. Patients often still require reading glasses.”
Even if implanted lenses do one day become good enough to put a damper on the post-cataract glasses market, optometrists will still be needed for their expertise in vision testing and patient counseling preoperatively. Bringing our refractive expertise to the table on this component of the surgical experience will position ODs to be an essential part of vision correction no matter how it’s achieved.
Dr. Donnenfeld says, “The next big thing in presbyopic IOLs will be true accommodating IOLs that give quality vision at near and far without an increase in glare and halo.” Several of these lenses, notably Juvene (LensGen) and PowerVision (Alcon), will enter FDA clinical trials in 2021, he notes.
Interestingly, Dr. Donnenfeld says the biggest optical challenge to optometry will not be presbyopic IOLs but the increased accuracy of distance-correcting IOLs, eliminating the need for distance correction and allowing the patient to wear over-the-counter readers. “My advice to my optometric colleagues is to embrace comanagement of cataract surgery, as this will continue to grow and ophthalmologists will appreciate the care our optometric colleagues can provide,” says Dr. Donnenfeld.
What about recent presbyopia-correcting eye drops that are making headlines? The question remains whether or not this will be another thorn in optometry’s side. Dr. Donnenfeld says, “Presbyopia-correcting drops are an exciting new pharmacologic approach to improving near vision. They essentially come with two different approaches: lens-softening drops, which still require a good deal of investigation, and miotics that improve depth of field.” Several miotics are entering phase II and III clinical trials and should be available in the near future, potentially as soon as this fall.
“The question that is raised is whether they’ll replace optical correction for near, and the short answer is no,” says Dr. Donnenfeld. “Yes, presbyopia drops will dramatically improve near vision, but they often will also mildly reduce the quality of vision at distance, especially when given in both eyes. Furthermore, presbyopia-correcting drops are short-term solutions. For many reasons, these pharmacologic approaches to presbyopia will be successful, and for just as many reasons, patients will still require optical correction when the miotics are not sufficient or appropriate to use.”
In Dr. Donnenfeld’s opinion, these drops will serve as a tool for eye care providers and should be embraced to improve patient quality of life and offer a new revenue source for practices.
Dr. Silverman agrees. “Each type of drop likely has pros and cons,” he says. “While I do believe these drugs can make it into the mainstream for treatment and management of presbyopia, for those concerned about lost revenues in optical sales from reading glasses, bifocals and/or progressive lenses, I wouldn’t close up the optical shop just yet!”
11 Lessons for a Bright, Prosperous FutureBy Randall Thomas, OD, MPH 2. Sincerely consider the Golden Rule as you interact with patients. 3. Commit to taking care of nearly all patients who come to you; said another way, commit to dramatically decreasing your referrals. 4. Meet with area physicians to introduce yourself and explain what you can do to partner with them to enhance patient care. 5. Tell every patient you see that you are a “real” eye doctor, and say to them, “Call me first with any eye problem you might have.” There is the perception that optometrists only spin dials and fit eyeglasses and contact lenses. Enough is enough. You have to share your story (and relay your expertise and training) with every patient. Your surgical counterparts certainly tell their patients the same thing. 6. If you have a dental emergency, you have the expectation that if you call your dentist’s office, they or a member of their call team can be reached and you’ll get the care you need. Why on earth should patients not expect the same from their eye doctor? We have to educate them that we do really care, and we demonstrate that by being accessible. 7. Visit all your local Urgent Care facilities, explain to them that you are available to help them with their patients with eye/vision problems, and leave business cards. Be available, or partner with area optometrists to share such 24/7 optometric availability. 8. Let area rheumatologists know you have expertise in Plaquenil evaluations. (Of course, make sure you can deliver on that.) 9. Meet with area primary care physicians and educate them on your expertise in diabetic retinopathy assessment. There is a huge unmet need out there, and us playing a large role in this clinical arena would be beneficial to all interested parties. 10. Subscribe to the journals Ophthalmology, American Journal of Ophthalmology and JAMA Ophthalmology. Until we all seriously apply ourselves to reading such journals, we will never attain the level of expertise that our patients expect us to have. We all already have access to optometric magazines, but extending our range of journal reading is absolutely critical to true professional growth. 11. Our offices must have an OCT, a state-of-the-art perimeter and a pachymeter. You just can’t provide physician-quality medical eye care without them. |
Make the Most of Medical
Cautiously adopting new advances after careful consideration, showing the value of high quality, in-person care and doing what we can to make up for dwindling optical and contact lens sales due to outside competitors are just a few of the ways optometrists are adjusting their sails to the changing winds in optometry. Luckily, for years now—since even before the advent of DPA/TPA certification—optometry as a profession has worked hard to push forward and expand its scope to become more medically driven in order to use the high level of education that ODs receive and maintain through their CE courses and training instead of primarily relying on optical revenue.
“The need for optometry to take on even more medical-based care is there,” says Randall Thomas, OD, MPH, of Concord, NC. “While there are currently numerous attacks on traditional optometry from many sides, there is also an enormous unmet need for medical eye and vision services,” he notes. “You have the opportunity to be proactive now, or panic when traditional optometric services are being done by non-optometrists, leaving the traditional types wondering what happened.
“As they say, ‘The times, they are a-changing.’ Be prepared to enjoy the fullness of being a forward-thinking, progressive medical eye doctor. The choice is yours, but with each passing year, the window of opportunity is narrowing. So, let’s get to work!”
Dr. Murphy has been a freelance science writer for 11 years. She received the Communications Award from the New York State Optometric Association for her writing in 2013. She is a graduate of SUNY College of Optometry and practices at Sachem Eye Care in Lake Ronkonkoma, NY. She has no financial interests to disclose.
