 |
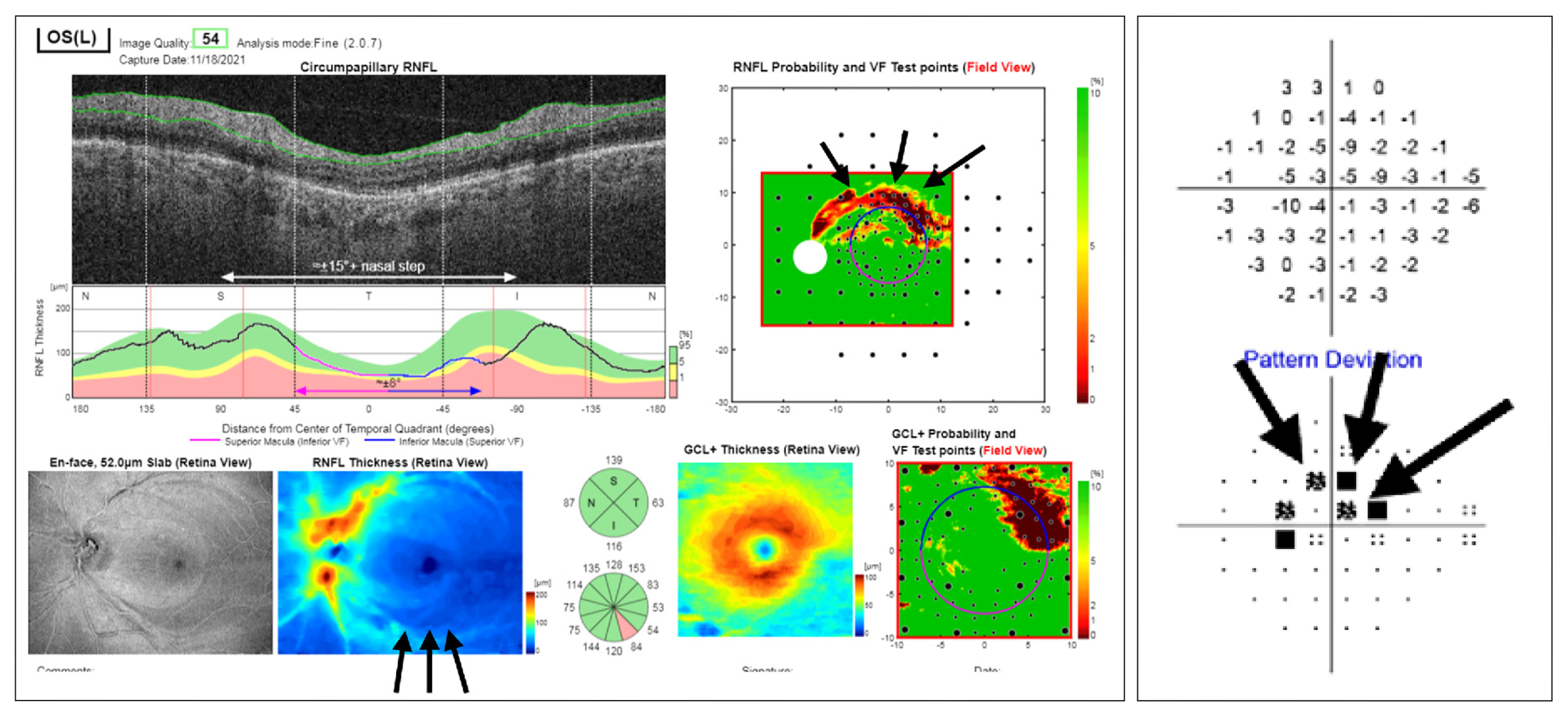
| Using a classification based on the fifth percentile, as is used in clinical practice, RNFL was shown to be superior to BMO-MRW in terms of sensitivity in glaucoma diagnosis with large optic discs. Photo: Jarett Mazzarella, OD, and Justin Cole, OD. Click image to enlarge. |
OCT of the optic nerve head (ONH) is an objective method that allows the early identification of this structural damage so that serious visual impairment can be prevented via the early initiation of treatment. Bruch’s membrane opening–based minimum rim width (BMO-MRW) and peripapillary RNFL are frequently used in clinical practice, and understanding of the diagnostic performance of these parameters in the detection of glaucoma is largely derived from receiver operating characteristics (ROC) analysis.
However, BMO-MRW can vary as a function of BMO size: Eyes with smaller disc sizes will be expected to have thicker MRW measurements as compared with eyes with larger disc sizes given the same number of ganglion cells. This raises the question of whether the ROC analysis reflects the actual performance in everyday clinical practice in eyes with small and large optic discs. In clinical practice, the classification of healthy and diseased participants is based on using the manufacturer’s fifth percentile as a threshold.
Researchers in Germany recently analyzed the performance of RNFL and BMO-MRW in glaucoma detection using both ROC analysis and classification based on percentiles depending on optic disc size. They found that, in eyes with large optic discs (BMO areas > 1.95mm2) and using the fifth percentile as a threshold, the sensitivity of BMO-MRW was inferior to that of RNFL for both early and moderate/advanced glaucoma.
The team assessed 100 eyes from 100 patients with early glaucoma (MD <-5.0dB) and 100 eyes from 100 patients with moderate/advanced glaucoma (MD >-5.0dB) were carefully matched to healthy controls based on optic disc size. The dataset was then divided, based on the 50th percentile of the measured BMO area into small (< 1.95mm2) and large optic discs (> 1.95mm2).
In discriminating between glaucoma and matched healthy controls, global BMO-MRW and global RNFL thickness had comparable areas under the ROC curve for eyes with early glaucoma and both small BMO areas (ROC: 0.91 and 0.88) and large BMO areas (ROC: 0.86 and 0.84), as well as in moderate/advanced glaucoma with small BMO areas (ROC: 0.99 and 0.97) and large areas (ROC: 0.94 and 0.97).
Using the calculated fifth percentile as a threshold value, the sensitivities for the detection of early and moderate/advanced glaucoma were comparable for BMO-MRW and RNFL in eyes with small optic discs (early glaucoma: 52% and 61%; moderate/advanced glaucoma: 91% and 92%). In eyes with large optic discs, the sensitivity of BMO-MRW was inferior to that of RNFL for both early (38% vs. 51%) and moderate/advanced (80% vs. 91%) glaucoma. The subgroup analysis of optic discs with a BMO area above 2.35mm2 showed a similar result.
“Both age and optic disc size are included in the calculation of the fifth percentile,” the researchers wrote in their paper. “This has the advantage of being more independent from the study population analyzed.”
The study suggested that the BMO-MRW is thinner overall in large optic discs, as the axons entering the optic nerve head are distributed over a wider rim area. Therefore, large but healthy discs may be erroneously classified as glaucomatous. “This, however, leads to a decrease in specificity—not in sensitivity—and only explains why many patients with large optic discs are classified as diseased in clinical practice, even though they are healthy, whereas a decrease in sensitivity is not explained,” the authors wrote.
“Our findings underscore the importance of RNFL imaging and measurement in the diagnostic evaluation of glaucoma, especially in eyes with large optic discs and a BMO area above 2.35mm2,” they concluded.
Englmaier VA, Stopr JJ, Leclaire MD, et al. Accuracy of Bruch’s membrane opening minimum rim width and retinal nerve fiber layer thickness in glaucoma diagnosis depending on optic disc size. Graefes Arch Clin Exp Ophthalmol. January 19, 2024. [Epub ahead of print]. |
