 |
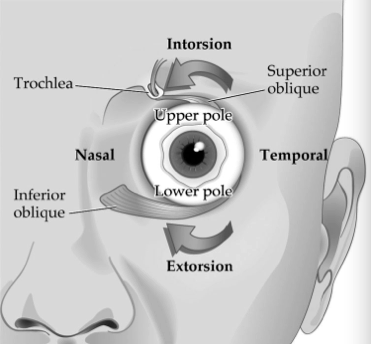
| Patients with ocular torsional instability but no signs of infantile or early-onset strabismus may require neuroimaging to rule out neurovestibular or cerebellar disease. Photo: www.quizlet.com. Click image to enlarge. |
A small study recently investigated how ocular torsional instability (OTI) can indicate the potential presence of prenuclear ocular motor dysfunction. The lead researcher concluded that in patients with OTI and preexisting strabismus, the condition appears to signify an infantile onset rather than the presence of an additional neurologic disease; however, the absence of infantile or early-onset strabismus may prompt the need for neuroimaging to rule out neurovestibular or cerebellar causes of prenuclear disease.
The retrospective chart review included 20 patients diagnosed with OTI, which was determined using indirect ophthalmoscopy. The researcher noted that eight patients had neuro-ophthalmologic disease caused by structural injury to prenuclear ocular motor areas; of these, six had structural lesions primarily involving the cerebellum, one had a midbrain glioma and one had traumatic encephalomalacia.
Additionally, eight other patients in the study cohort had infantile strabismus (esotropia in seven and exotropia in one) “associated with various combinations of monocular nasotemporal optokinetic asymmetry, latent nystagmus and dissociated vertical divergence, indicating prenuclear involvement of subcortical visuovestibular pathways within the brain,” the researcher reported in his paper on the study, published recently in the Journal of Neuro-Ophthalmology.
Three OTI patients presented with intermittent exotropia with dissociated vertical divergence, which the researcher noted suggests an early onset. Two other patients had acquired esotropia that developed after infancy. One of these had partially accommodative esotropia with bilateral inferior oblique overaction, and the other had acquired esotropia followed by spontaneous secondary exotropia.
After analyzing the data, the study author made several conclusions in his paper. “OTI is useful in diagnosing coexistent prenuclear disease in patients with unilateral or bilateral superior oblique palsy,” he wrote. “Clinically, it differs from the torsional instability of superior oblique myokymia in that it is bilateral and symmetrical and not accompanied by oscillopsia.” He points out that “owing to its small amplitude and the inability to examine both eyes simultaneously (without eye movement recordings), it is usually impossible to confirm whether this binocular torsional instability is conjugate. The fact that OTI is conspicuously absent in nuclear and intranuclear disorders such as ocular nerve palsies, however, makes it an important neurodiagnostic sign to recognize when present.”
In order to recognize OTI and use the finding to diagnose prenuclear disease, several steps must be properly orchestrated during the exam. “First, the indirect ophthalmoscopy light source must be turned to a low level that still allows adequate retinal visualization because the patient is asked to look at the light to stabilize fixation,” the author explained in his paper. Because patients with severe vision loss are unable to fixate, it may not be feasible to assess for OTI in this population.
The author cites four additional considerations for assessing OTI in patients:
- It’s important to distinguish OTI from fixation instability, which confers a momentary variability to the foveal position that disrupts fixation.
- The presence of nystagmus makes OTI more difficult to diagnose, as the larger movements it produces can obscure more subtle torsional rotations in OTI.
- OTI commonly accompanies latent nystagmus or dissociated vertical divergence; however, it may also appear in the absence of these conditions in patients with infantile strabismus.
- When dissociated vertical divergence is present, OTI can accompany intermittent exotropia with normal stereoacuity, suggesting an infantile origin for these cases.
In conclusion, the author notes that “OTI can be considered a useful clinical sign of prenuclear disease involving the ocular motor system.” Additionally, neuroimaging may particularly be warranted in patients without infantile or early-onset strabismus who present with OTI.
Brodsky MC. Ocular torsional instability—a neurodiagnostic sign of prenuclear disease. J Neuro-Ophthalmol. May 12, 2023. [Epub ahead of print]. |
