 |
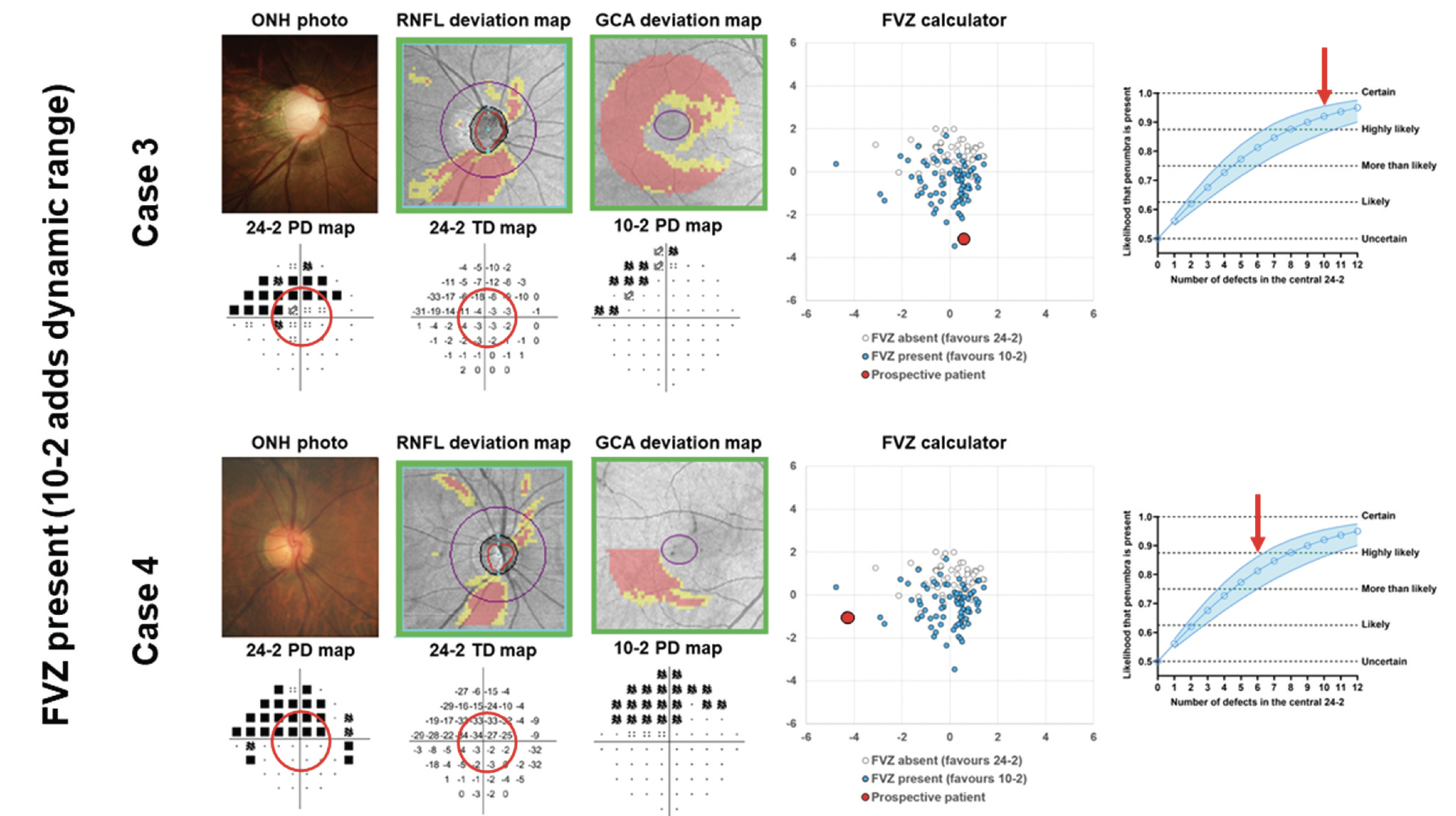
The FVZ in VF testing reflects a potential zone where residual VF sensitivity or test dynamic range, if captured, allows for ongoing monitoring of the glaucomatous VF defect. In these examples, an FVZ is likely to be present (red dots and red arrows). Photo: Phu J, et al. Clin Exp Optom. December 6, 2023. Click image to enlarge. |
Vulnerable patients who may benefit from the lesser used 10-2 perimetric modality can sometimes go unnoticed, as there is currently no paradigm outlining when to deviate from the standard 24-2 test. Authors of one new study conducted research to determine a method for 10-2 deployment in glaucoma, with the goal of detecting additional visual field (VF) sensitivity with the purpose of functional monitoring.
The study authors developed a pilot method to determine when to deploy the 10-2 VF test grid in glaucoma, characterized by what they called a “functional vulnerability zone” (FVZ). To do so, results from the cross-sectional 24-2 (central 12 locations) and 10-2 VF tests were collected from 133 glaucomatous eyes. These eyes were used to describe the central hill of vision using VF sensitivity. The ‘volume’ under the hill was calculated using arbitrary units, with greater number of units on the 10-2 test indicating the FVZ that signifies additional clinical dynamic range for potential future monitoring.
The researchers found that over 55% of patients had an FVZ, more so using 10-2 over 24-2. The FVZ group displayed several 24-2 features that were significant when compared with the non-FVZ group, including worse mean deviation, worse central 24-2 mean defect and a higher proportion of defective locations. 10-2 may be applicable at low 24-2 mean deviation levels, ranging in favor from -3.2dB to -3.6dB. More concretely, five or more defective central 24-2 test locations were associated with an FVZ. Finally, those who exhibited less severe defect on the 10-2 were more likely to have an FVZ, indicating a potential use for future VF monitoring.
In their paper the authors elaborated on their data, adding that in cases where no FVZ was observed, the 10-2 test grid adds theoretically little additional useful information in respect to dynamic range. However, the strongest relationship indicating 10-2 usefulness was with the proportion of defects found centrally (i.e., five or more of the 24-2 test locations).
Using these parameters, the authors devised two aids. One is a pilot-data derived, downloadable spreadsheet to help clinicians decide when to employ the 10-2, based on the likelihood of an FVZ being present. The other is a simplified predictor of whether an FVZ is likely to be present, based on the number of affected 24-2 test central locations.
Contextualizing their aids, the authors propose that “this pilot spreadsheet aims to address gaps in the knowledge where there is no clear quantitative metric guiding when a 10-2 would provide additional dynamic range compared to the 24-2. For this reason, the spreadsheet utilizes both 10-2 and 24-2—effectively paired—data to identify, within patient, the FVZ.”
They do mention that the spreadsheet is not meant to be prescriptive, explaining why they did not include a clearly defined FVZ boundary. Instead, they argue, “its purpose is to guide the clinician as to the likelihood or probability, based on the distribution of results, of the 10-2 test grid facilitating the future monitoring of residual visual field sensitivity.”
Phu J, Rafla D, Kalloniatis M. Which glaucoma patients benefit from 10-2 visual field testing? Proposing the functional vulnerability zone framework. Clin Exp Optom. December 6, 2023. [Epub ahead of print]. |
