11th Annual Cornea ReportThe April 2024 issue of Review of Optometry highlights some hot topics in cornea, from keratoconus assessment and monitoring, to advancements in endothelial surgery, to causes and treatments of corneal pain. Check out the other articles featured in this issue:
|
If you are like me and regularly find yourself evaluating topographical maps, you have probably had a variety of thoughts. When starting out in an academic setting, you might have asked yourself: What do these values mean? Which numbers should I pay the most attention to? How do I diagnose conditions based on these maps? Which patients need to have a scan performed on their corneas? Eventually in practice, you may be wondering: Which instrument is worth the money? Which data is reliable, and which is misleading? Now that I have the basics, where can I take this data further in my patient care?
This article will answer questions that help distinguish how to best use these devices or read the data.
Instrumentation
In a market where there are so many different options to evaluate data, it can be difficult to discern which options are truly necessary and where clinical data can become misleading. It is important to differentiate between corneal topography and corneal tomography scans. Corneal topography and corneal tomography serve as crucial diagnostic tools, and each offer distinct insights into the structure of the cornea. More commonly, you will likely encounter corneal topography instruments in your average practice setting due to its accessibility and lower cost. Corneal topography focuses on the anterior surface, providing a detailed two-dimensional map of its curvature and identifying irregularities such as corneal astigmatism. This method is valuable for assessing refractive errors and aiding in the planning of corrective procedures.
In contrast, corneal tomography goes beyond surface analysis, offering a comprehensive three-dimensional representation of the entire cornea. This includes details about corneal thickness and the posterior surface, making it particularly useful for detecting conditions such as subtle keratoconus and other corneal ectasias. Corneal tomography provides a holistic assessment of corneal structure and aids in early detection of pathological changes that corneal topography instrumentation may not provide. Therefore, while corneal topography excels in surface analysis, corneal tomography offers a three-dimensional perspective vital for a thorough evaluation of the cornea’s structure.
There are three main types of imaging devices used to perform corneal topography and corneal tomography scans: Placido disc devices, Scheimpflug imaging and anterior segment OCT (AS-OCT). While the latter reveals what type of corneal scan it can produce based on the name itself, it is important to delve into each one of these machines to understand how they capture information and to determine which one makes the most sense for your practice setting needs.
Placido Ring Corneal Topography
These corneal instruments are widely used for corneal topography and not tomography assessments. These devices use a specific optical technique based on the principles of the Placido disc, named after Antonio Placido, who first described using a circular target with alternating concentric dark and light rings with a central aperture to photograph and observe the corneal reflections they produced in 1880.1
The Placido disc that we use today still consists of a series of concentric rings or circles that are illuminated and reflected off the cornea. As the rings are projected onto the cornea’s surface, they create a distinct pattern of bright and dark areas. The instrument’s camera captures this pattern and analyzes the reflected image to derive information about corneal shape and curvature.1
The measurement of corneal topography with Placido ring instruments relies on the distortion of the reflected ring pattern on the cornea. When the cornea is smooth and regular, the reflected rings are also smooth and symmetric. However, irregularities or abnormalities of the corneal surface cause distortions in the ring pattern. By assessing these distortions, the instrument can create a detailed map of the corneal surface and highlight areas of curvature variation and abnormalities.
One notable advantage of Placido ring corneal instruments is their noninvasive nature and efficiency in providing quick and accurate corneal topography measurements. Additionally, these instruments have been integral in enhancing the precision of refractive surgeries, as they allow eyecare professionals to tailor treatments based on the individualized corneal characteristics revealed by the topography maps. Practitioners can obtain pre-surgery assessments, customize ablation profiles and follow up post-surgically. For practitioners who prescribe specialty contact lenses, especially for gas permeable contact lenses such as orthokeratology, this device’s advancements have allowed different contact lens fitting software programs to screen simulated fluorescein patterns, calculate contact lens parameters and more.1 These devices are even capable of performing dry eye assessments due to the noninvasive keratography dry-up time that can be measured because of the device’s dependence on tear film.2
While Placido ring corneal topography remains a valuable tool in practice, it has some limitations and disadvantages. First and foremost, the Placido ring instrument does not provide posterior surface information since it focuses on the anterior surface of the cornea.1 This limitation may be incredibly significant in conditions where abnormalities or changes occur in the posterior cornea.
Second, the accuracy of Placido ring corneal topography is dependent on the quality of the tear film on the cornea. Tear film irregularities, such as dry spots or debris, may lead to distorted measurements, which impacts corneal map reliability.
Third, Placido ring technology can tend to struggle with cases of highly irregular corneas in providing accurate and detailed maps. The distortion of the ring pattern on severely irregular corneas can make it challenging to obtain precise measurements.
Fourth, this type of corneal topography does not provide information on corneal thickness. For conditions like keratoconus and glaucoma, where measuring pachymetry is crucial, an alternative instrument is needed to provide the patient treatment and management data. While the technology remains widely used and effective, eyecare professionals need to know these limitations in order to consider complementary diagnostic methods with specific corneal conditions or irregularities.
Overall, Placido ring corneal instruments play a vital role in modern ophthalmic practice by offering valuable insights into corneal structure and aiding in the diagnosis and treatment planning for a variety of eye conditions. More sophisticated Placido ring devices are now being combined with Scheimpflug imaging or scanning-slit technology to improve the relevance and use when imaging the cornea.3
Scheimpflug Imaging
These advanced imaging instruments are employed for the precise measurement of corneal tomography. Named after the Austrian physicist Theodor Scheimpflug, these devices use a unique optical principle to capture detailed 3D images of the entire cornea.1 Unlike Placido ring topography, Scheimpflug devices excel in providing comprehensive data, including data for anterior and posterior corneal surfaces as well as corneal thickness. The technology relies on a tilted camera that captures images along the Scheimpflug principle which ensures that both the cornea and lens are in sharp focus simultaneously and results in highly-detailed tomographic images.1
There are three commonly used Scheimpflug devices: Pentacam (Oculus), Galilei (Ziemer Ophthalmic Systems) and Sirius (Schwind). The former uses a single rotating camera and a static camera, while the latter two combine a Placido topographer with a single- and a dual-rotating Scheimpflug camera.3
One significant advantage of Scheimpflug devices is their ability to assess the entire cornea and offer a wealth of information for diagnostic and surgical planning purposes. These devices provide detailed maps of corneal thickness, which is crucial for detecting subclinical or early keratoconus and refractive surgeries. Scheimpflug imaging can detect subtle changes in corneal structure, which makes it valuable for monitoring disease progression and evaluating treatment outcomes. The obtained three-dimensional data enhances assessment precision and accuracy and contributes to improved clinical decision-making. The Scheimpflug principle helps capture data from the peripheral cornea that centrally-located scanning slit-based cameras are not as capable of.3
Despite their advantages, Scheimpflug devices also have limitations in certain cases. They require precise fixation and alignment from the patient during image acquisition. In cases of poor fixation or uncooperative patients, obtaining reliable and accurate images may be challenging and could lead to data inaccuracies. Furthermore, the presence of dense cataracts or corneal opacities can limit Scheimpflug imaging effectiveness.3 These opacities may obstruct the passage of light through the cornea, resulting in suboptimal images and reduced visibility of corneal structures. Also, these devices can be costly, with the initial investment, maintenance and training costs potentially posing financial challenges for some healthcare facilities. Depending on the region you reside in, availability of these devices may also be limited. If a full three-dimensional analysis of the cornea is desired, obtaining these Scheimpflug images can be time-consuming compared with other corneal imaging methods, since multiple images will need to be taken from different angles before it is analyzed by the system.3
Even with these limitations, Scheimpflug imaging remains a cutting-edge technology with significant advantages in corneal tomography. Its ability to provide detailed information about corneal structure, including thickness and curvature, makes it a valuable tool for diagnosing and managing various eye conditions.
AS-OCT
The final corneal imaging device we will be discussing is AS-OCT. This is a non-invasive imaging technique that has emerged as a valuable tool for measuring corneal tomography. This technology uses low-coherence interferometry to generate high-resolution, 3D images of the cornea, allowing for a comprehensive assessment of its structure.4
Currently, there are two main types of OCTs: Fourier-domain and time-domain. Time-domain OCT varies the position of a reference mirror to create cross-sectional images, whereas Fourier-domain OCT has a fixed mirror and relies on an interference between the reference and sample reflections.3 Fourier-domain has a faster acquisition time than time-domain, which helps Fourier-domain reduce motion artifacts from patients’ eye movements and provide better resolution.3
A key advantage of AS-OCT in corneal tomography is its ability to provide detailed information about both the anterior and posterior surfaces of the cornea as well as corneal thickness. This comprehensive data is crucial for diagnosing and managing conditions of keratoconus, corneal dystrophies and for preoperative planning in refractive surgeries. AS-OCT enables clinicians to visualize corneal layers with exceptional detail and gain insights into subtle changes in corneal morphology that may not be apparent with other imaging modalities. Another advantage is image acquisition speed, which allows for quick and efficient examinations.4 However, it is important to note that factors such as proper alignment and fixation are still critical for obtaining accurate measurements with AS-OCT.
While AS-OCT offers numerous advantages in measuring corneal tomography, like the other devices, it is not without its limitations and disadvantages. First, AS-OCT may have limited penetration depth, depending on the presence of corneal opacities or conditions that lead to incomplete visualization of deeper corneal layers.4 Therefore, obtaining detailed images of the entire cornea may be challenging. AS-OCT images are highly susceptible to artifacts, which can present due to a variety of factors, such as blinking or motion.4 Moreover, these devices are moderately expensive and its accessibility can be prohibitive depending on budget constraints. Further, inexperienced operators might face challenges obtaining accurate and reliable measurments. Finally, AS-OCT typically provides a limited field of view per scan taken compared with the other two modalities and it is more tedious to scan the entire cornea if desired.4
Better When Used Together
While Placido ring devices are focused on corneal topography, both Scheimpflug imaging and AS-OCT provide comprehensive corneal tomography. The choice between them depends on your clinical requirements, level of detail needed and factors of cost and availability. To follow are cases where reliance on solely one modality might be clinically misleading, as each technique has its limitations. Here are some scenarios where the use of one imaging device alone may not provide a complete or accurate picture.
Keratoconus detection. Placido ring devices may not be as sensitive in detecting early or subtle cases of keratoconus, as they do not offer posterior elevation or corneal thickness measurements.5 For patients with moderate to high astigmatism measured on Placido ring devices, it may be warranted to employ additional testing with techniques of Scheimpflug imaging or AS-OCT. However, due to the high cost of Scheimpflug imaging devices such as Pentacam, there is an argument for the expansion of corneal topography scans to be completed more often as part of the routine comprehensive examination. Regardless of the imaging device that you have access to, it is critical to image these subsets of patients to detect corneal disease as early as possible. Advanced cases with significant irregularities might also be better visualized with more detailed Scheimpflug imaging or AS-OCT.
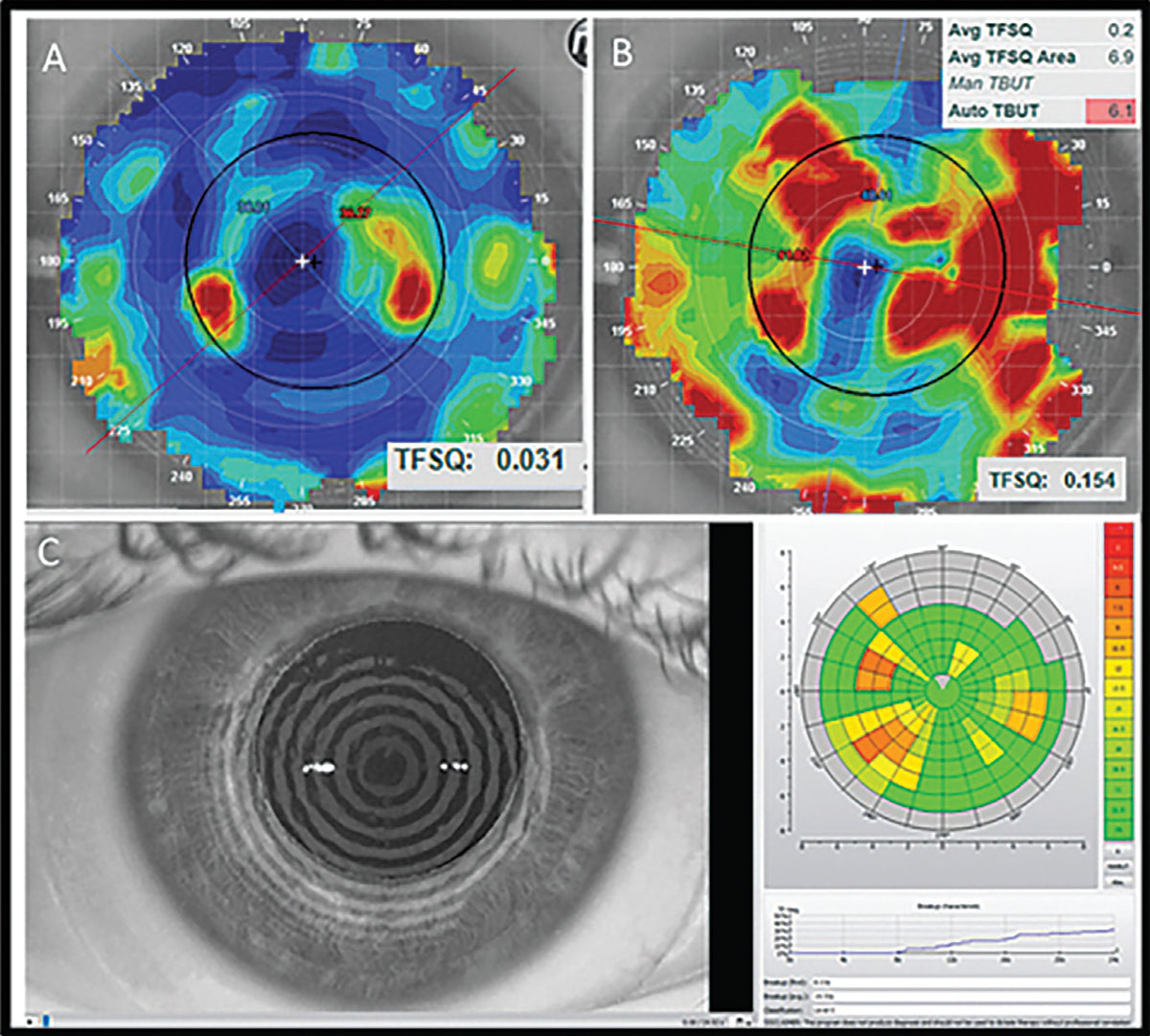
Tear film instability. Placido ring devices may also result in misleading data from meibomian gland dysfunction prevalence, depending on the patient.6 Since Placido ring devices are tear film dependent, an unstable tear film may result in misleading information on the imaging results. Figure 1 shows an example of noninvasive tear breakup assessments.
 |
|
Fig. 1. The top panel shows the tear film quality score display from an E300. The bottom panel is a similar assessment using the keratograph. Photo: Maria Walker, OD. Click image to enlarge. |
It is therefore imperative to remember what each device relies on to develop its images prior to sending the patient for image acquisition. For example, if it is already evident upon slit lamp examination that the patient has decreased tear meniscus or decreased tear break-up time, it may be helpful to instill a drop of artificial tears prior to sending the patient for a corneal topography scan with a Placido disc device. In practice settings where testing is done prior to slit lamp examination, optometric technicians can be trained to look for clear mires and to capture images just after blink to minimize the tear film dependency of Placido ring imaging devices.
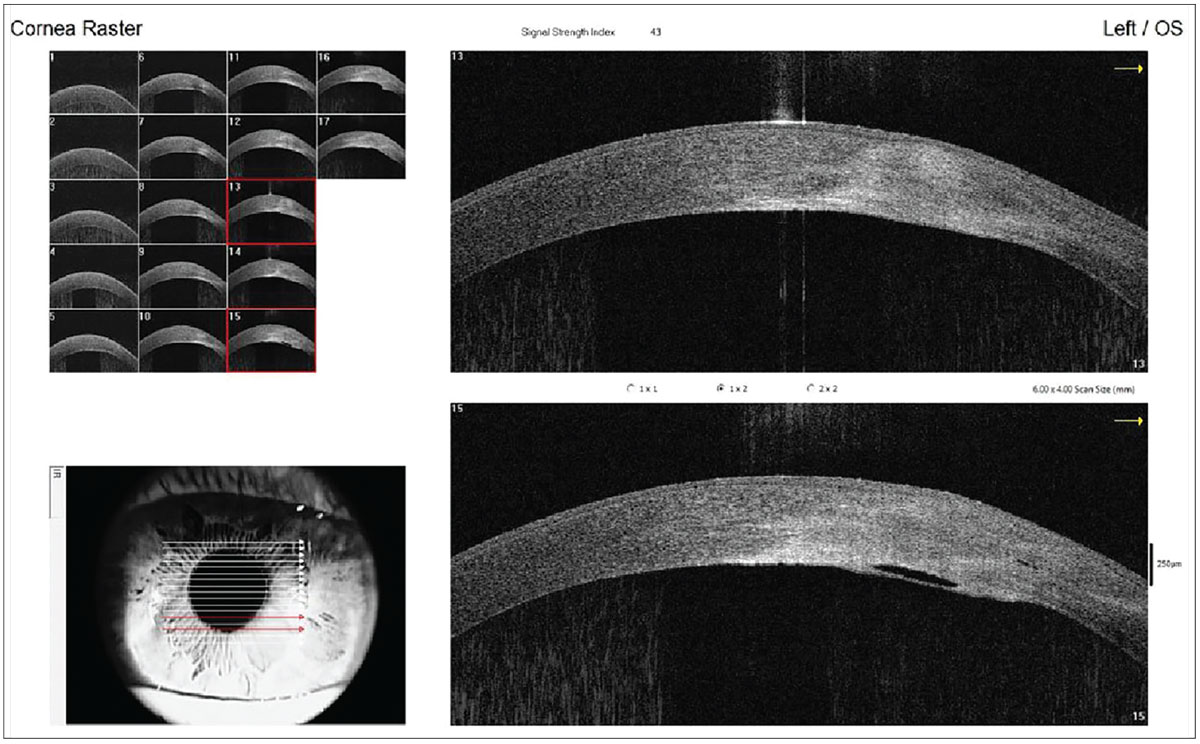
Dense corneal opacities. Deeper layers of the cornea can potentially be missed when viewed on an AS-OCT.4 If only the anterior surface of the cornea can be adequately imaged due to the density of the opacity, then areas of the posterior cornea may be missed, despite the device’s capabilities as a corneal tomographer. Figure 2 shows an AS-OCT image of a resolving corneal hydrops in a patient with keratoconus.
 |
|
Fig. 2. This AS-OCT image highlights corneal edema and the break in Descemet’s membrane. If there was a dense surface opacity here, the break might have been missed. Photo: Sharon Keh, OD, Irene Frantzis, OD, and Yana Seviaryn, OD. Click image to enlarge. |
Posterior segment abnormalities. While Scheimpflug imaging provides excellent information about the anterior and posterior corneal surfaces, it may not capture details of abnormalities in the posterior segment of the eye beyond the cornea. OCT may be necessary to appropriately image posterior segment findings. Conditions that affect the lens or the posterior chamber may not be fully assessed. This, however, can be remedied by a multimodal imaging approach.
In clinical practice, a multimodal imaging approach is often preferred to overcome the limitations of individual techniques. Combining Placido ring devices, Scheimpflug imaging and AS-OCT allows for a more thorough evaluation of the cornea and anterior segment, enhancing the clinician’s ability to make accurate diagnoses and informed treatment decisions. Integrating clinical judgment with data from multiple sources ensures a more comprehensive understanding of the patient’s ocular health. However, this may not always be possible, depending on the budget and technology available in each practice setting. Considering that corneal topography and corneal tomography are both billed under the same Current Procedural Treatment (CPT) code—92025—it may be difficult to purchase a significantly more expensive imaging modality, depending on patient population and practice setting.
Even so, there is the potential for variability of posterior corneal surface and thickness measurements between Placido-Scheimpflug and swept-source OCT imaging.7 There are relatively consistent measurements of horizontal white-to-white and horizontal-vertical iris diameter within each imaging device, but be aware of significant variability when comparing between devices.8 Consequently, the benefits of using multimodal imaging for our patients when trying to discern a proper diagnosis may not carry over when using Scheimpflug-based and OCT-based imaging interchangeably when trying to monitor progression or changes over time.9
Assessing Keratoconus
When considering multimodal imaging options, consider that the different grading systems for keratoconus specifically vary depending on the instrument used. When using the Amsler-Krumeich grading scale, for instance, the scale solely relies on corneal topography.10 The newer ABCD grading scale from Belin and Duncan consider additional factors of corneal pachymetry, both anterior and posterior corneal surfaces and best spectacle-corrected visual acuity.11,12 Many of these measurements need data from a corneal tomographer to adequately assess the patient on the ABCD grading scale.5
In terms of risks and benefits for using one imaging modality over another, there are studies showing that patients with keratoconus who have corneal tomography scans are more likely to undergo corneal collagen crosslinking.13-16 Early crosslinking may lead to a need for fewer future keratoplasties, and early detection of keratoconus in conjunction with preventative treatment measures can prevent needing more invasive surgical methods.13-16
To adequately differentiate between clinical and subclinical keratoconus, the imaging devices measure various parameters to help the practitioner reach a more definitive diagnosis.
Table 1 provides a list of parameters measured by corneal tomographers that can help indicate to the practitioner the presence of definitive keratoconus.
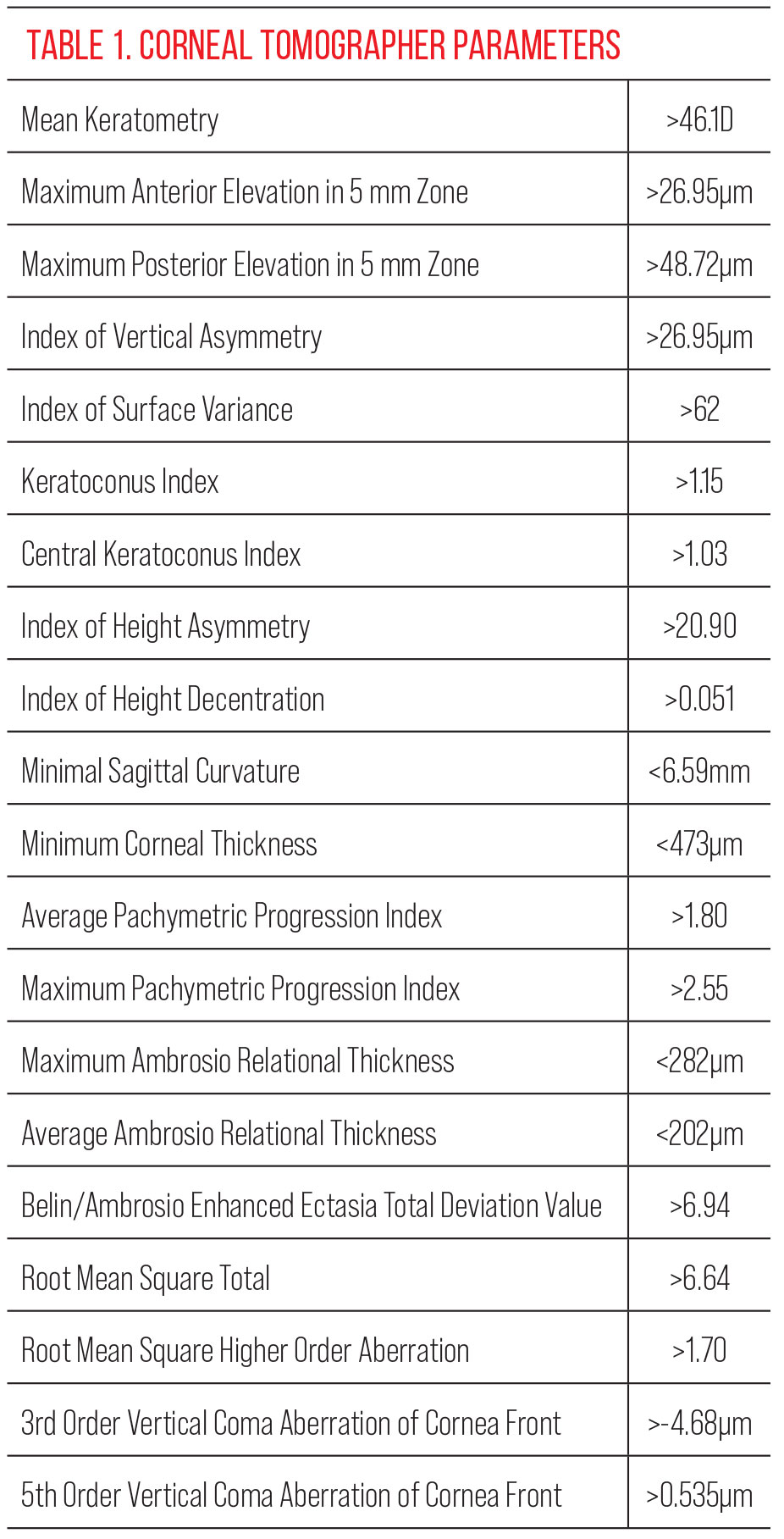 |
| Click image to enlarge. |
There are various studies in the literature that point to which diagnostic indices are the most impactful in diagnosing clinical and subclinical keratoconus. The more recent studies were primarily performed on the Pentacam. One in particular measured the Belin/Ambrosio Deviation Display, the fifth order vertical coma aberration, the index of surface variance and the index of vertical asymmetry to be some of the most important indices to watch for in keratoconus diagnosis.17 For borderline diagnosis cases, Belin/Ambrosio Deviation Display values ≥1.54, fifth order vertical coma aberration of the front cornea ≥0.023, index of surface variance values ≥22 and index of vertical asymmetry values ≥0.14 should also raise suspicion for keratoconus.17
In another study, back maximum keratometry, index of vertical asymmetry, inferior-superior difference and root mean square total values were found to be the most accurate indices for diagnosing definitive keratoconus.18 The study also found that the values to pay close attention to for diagnostic indices with the best specificity and sensitivity for detecting subclinical keratoconus were index of surface variance, index of vertical asymmetry, keratoconus index, posterior radius of curvature, root mean square high order and back maximum keratometry.18 Multiple studies reported that the Belin/Ambrosio Enhanced Ectasia Display played a crucial role in detecting subclinical keratoconus.17-19
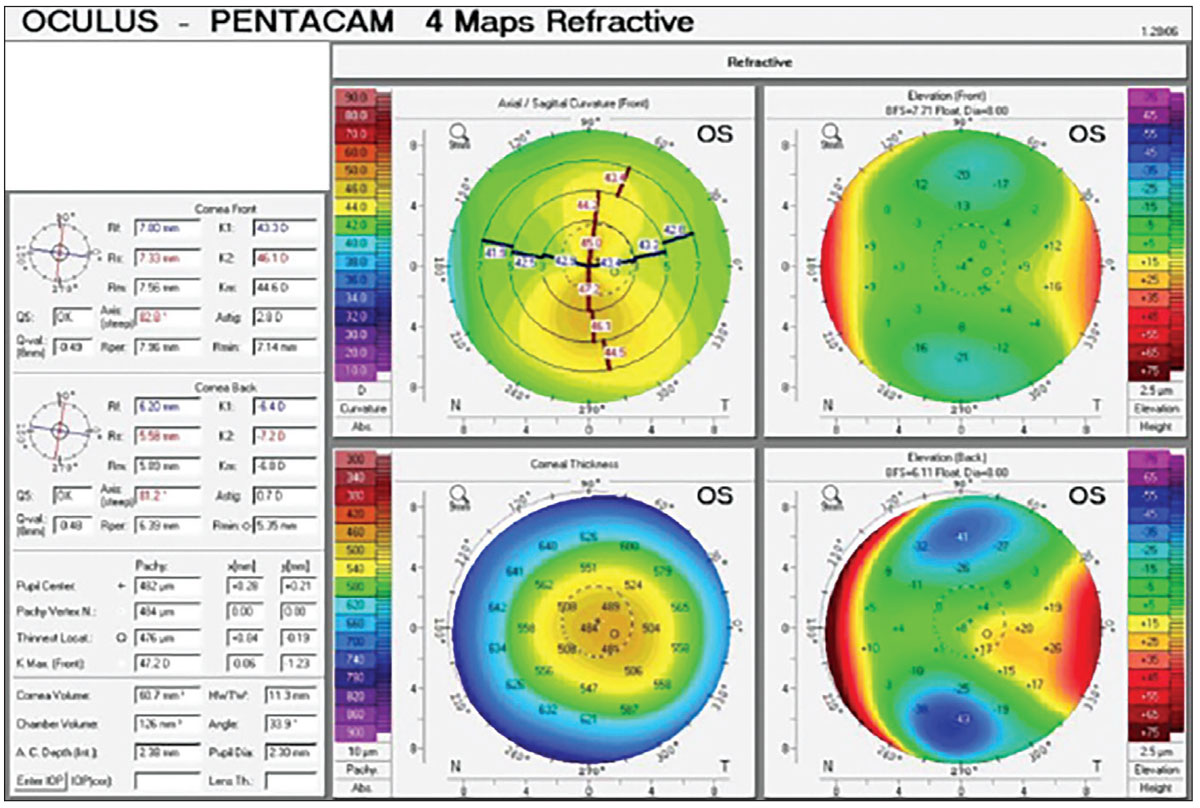
Here is an example of a patient whose refractive error not only showed high astigmatic correction, but the astigmatic correction was also asymmetric. She had no previous remarkable ocular history to note. A Scheimpflug image was taken, and the findings for her left eye are indicated in Figure 3.
 |
|
Fig. 3. Pentacam four maps refractive scan OS of a keratoconus suspect. Click image to enlarge. |
If we can pay attention solely to the axial front curvature map and the front elevation map, the cornea looks asymmetric, but depending on the device used, you might not automatically diagnose this patient with a specific condition. With the corneal tomography device, we are also able to obtain the pachymetry measurement, which indicates the patient has thinner than average corneas. When observing the back elevation map along with the front elevation map, you can compare how they look and whether the back elevation is steeper than the front elevation map to indicate ectasia.
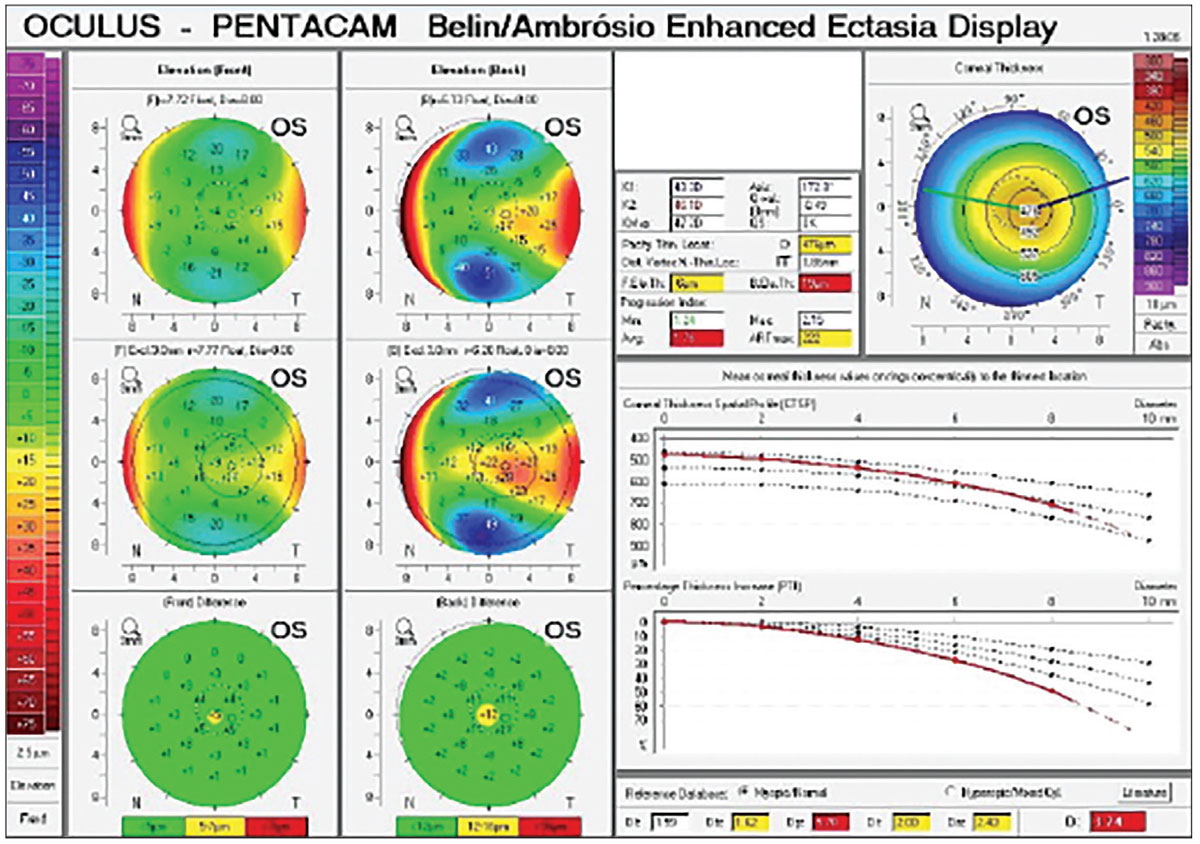
For the patient in Figure 4, it looks like only the central point shows a suspicious elevation difference. To the right, you can see a map of the pachymetry values at the apex of the cornea as well as at the thinnest point. Generally, the higher the displacement is of the thinnest pachymetry value from the apex, the more likely it is that the patient has keratoconus. As you can see in the top right panel of the image, there is some displacement of the thinnest pachymetry to the apex. On the bottom right, you can see graphs of the Corneal Thickness Spatial Profile (CTSP) and the Percentage Thickness Increase (PTI). The CTSP shows how the cornea progressively thickens from the thinnest point, and the PTI shows the percentage of increase in corneal thickness from the thinnest point to the peripheral cornea.20 Both graphs show a 95% confidence interval with the average normal population in the center.20
 |
|
Fig. 4. While the top two maps on the left show the standard and exclusion elevation maps that are used used to show the front and back elevation maps in relation to their best fit sphere. The bottom two maps show the elevation differences between front and back surface and will flag areas that are suspicious for greater differences than the norm.20 Click image to enlarge. |
Comparatively, this patient has a more rapid thickening and higher percentage of thickening than the normal population. Since patients with keratoconus have a more rapid progression of thickening from the thinnest point to the peripheral cornea, there is concern for early ectatic disease.
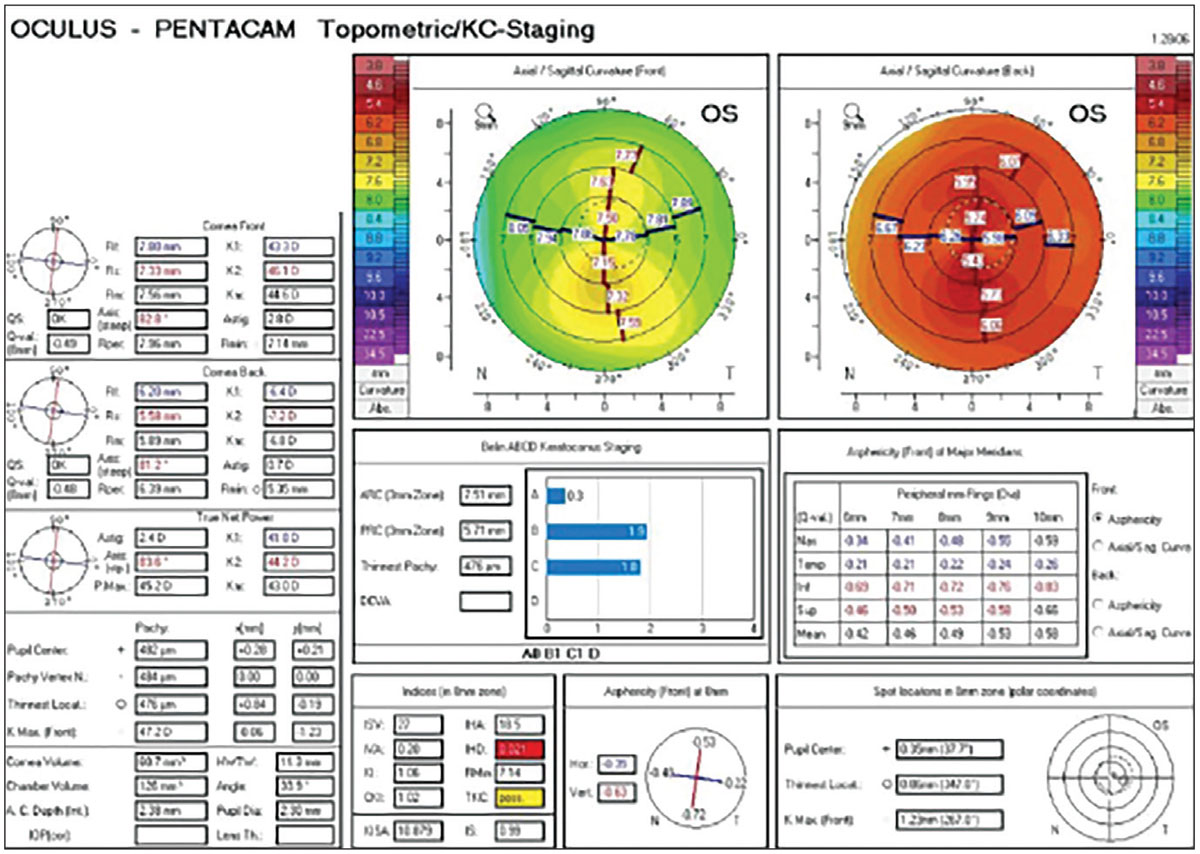
While there is no universally agreed-upon keratoconus staging method, the topometric/keratoconus staging, pictured in Figure 5, shows more information on the Belin ABCD Keratoconus Staging Method. It also offers more information on the asphericity of the front major meridians as well as indices within the 8mm zone of the cornea to evaluate.11 The ABCD system uses four parameters that are listed in the scan: anterior radius of curvature in the 3.0mm zone centered around the thinnest location, posterior radius of curvature in the same zone as the anterior radius, thinnest pachymetry in microns and distance best-corrected visual acuity.12
 |
|
Fig. 5. Pentacam topometric/keratoconus staging OS of a keratoconus suspect. Click image to enlarge. |
For this particular patient, the keratoconus staging shows that the patient’s posterior radius of curvature and the thinnest pachymetry are almost at stage 2. The index of height decentration is also considered significantly abnormal and flagged under indices. The Topographic Keratoconus Classification has this patient listed as possible for keratoconus.
At this point, while there is no clear definitive keratoconus clinically or under all the indices on the corneal tomography scan, there is suspicion for it. Once the patient returns for another corneal tomography scan, we will be able to use the Belin ABCD Progression Display to measure progression over time of the four parameters used in the Belin ABCD Keratoconus Staging Method.12
Takeaways
Interpreting corneal scans requires the clinician to have a nuanced understanding of the specific imaging modality used and the ability to discern clinically relevant information. Regular training and staying current in the advancements in imaging technologies are essential for eyecare professionals to enhance their interpretative skills. Collaboration with colleagues and consultation with cornea specialists can also be valuable in managing our most challenging cases.
Dr. Song earned her degree from the SUNY College of Optometry and stayed on to complete her residency in cornea and contact lenses with an emphasis in anterior segment and ocular disease. She graduated with the honors of the Chancellor’s Award for Student Excellence and the Johnson & Johnson Vision Award of Excellence in Contact Lens Patient Care. Upon residency completion, she became a fellow of the American Academy of Optometry and was the inaugural winner of the Visionary in Eye Care Resident Recognition Award in the “Best in Optometry” category. She currently serves on the GP Lens Institute Rising Stars Committee and is a participant in the American Optometric Association Leadership Institute. Dr. Song has delivered numerous COPE-approved lectures and presented many posters at academic meetings. She currently works at Fromer Eye Centers seeing specialty contact lens patients.
1. Martin R. Cornea and anterior eye assessment with placido-disc keratoscopy, slit scanning evaluation topography and scheimpflug imaging tomography. Indian J Ophthalmol. 2018;66(3):360-6. 2. Marx S, Sickenberger W. A novel in-vitro method for assessing contact lens surface dewetting: Non-invasive keratograph dry-up time (NIK-DUT). Cont Lens Anterior Eye. 2017;40(6):382-8. 3. Fan R, Chan TC, Prakash G, Jhanji V. Applications of corneal topography and tomography: a review. Clin Exp Ophthalmol. 2018;46(2):133-46. 4. Chong YJ, Azzopardi M, Hussain G, et al. Clinical applications of anterior segment optical coherence tomography: an updated review. Diagnostics (Basel). 2024;14(2):122. 5. Kong AW, Ahmad TR, Turner ML, et al. Trends in corneal topography and tomography imaging for keratoconus management. Clin Ophthalmol. 2022;16:1357-63. 6. Matossian C. Topography to screen refractive cataract surgery patients for OSD. CRST Global Europe Edition. crstodayeurope.com/articles/2015-may/topography-to-screen-refractive-cataract-surgery-patients-for-osd. Published May 2015. Accessed February 1, 2024. 7. Chan TCY, Biswas S, Yu M, Jhanji V. Comparison of corneal measurements in keratoconus using swept‐source optical coherence tomography and combined Placido–Scheimpflug imaging. Acta Ophthalmol. 2017;95(6):e486-94. 8. Boyle AB, Namkung S, Shew W, et al. Repeatability and agreement of white-to-white measurements between slit-scanning tomography, infrared biometry, dual rotating Scheimpflug camera/Placido disc tomography, and swept source anterior segment optical coherence tomography. PloS One. 2021;16(7):e0254832. 9. Schiano-Lomoriello D, Bono V, Abicca I, Savini G. Repeatability of anterior segment measurements by optical coherence tomography combined with Placido disk corneal topography in eyes with keratoconus. Sci Rep. 2020;10(1):1124. 10. Amsler M. [The “forme fruste” of keratoconus]. Wien Klin Wochenschr. 1961;73:842-3. 11. Belin MW, Duncan JK. Keratoconus: the ABCD Grading System. Klin Monbl Augenheilkd. 2016;233(6):701-7. 12. Belin MW, Kundu G, Shetty N, et al. ABCD: a new classification for keratoconus. Indian J Ophthalmol. 2020;68(12):2831-4. 13. Hersh PS, Greenstein SA, Fry KL. Corneal collagen crosslinking for keratoconus and corneal ectasia: one-year results. J Cataract Refract Surg. 2011;37(1):149-60. 14. Wollensak G. Corneal collagen crosslinking: new horizons. Exp Rev Ophthalmol. 2010;5(2):201-15. 15. Godefrooij DA, Gans R, Imhof SM, Wisse RPL. Nationwide reduction in the number of corneal transplantations for keratoconus following the implementation of cross‐linking. Acta Ophthalmol. 2016;94(7):675-8. 16. Sandvik GF, Thorsrud A, Råen M, et al. Does corneal collagen cross-linking reduce the need for keratoplasties in patients with keratoconus? Cornea. 2015;34(9):991-5. 17. Hashemi H, Beiranvand A, Yekta A, et al. Pentacam top indices for diagnosing subclinical and definite keratoconus. J Curr Ophthalmol. 2016;28(1):21-6. 18. Nicula CA, Bulboacă AE, Nicula D, et al. Performances of corneal topography and tomography in the diagnosis of subclinical and clinical keratoconus. Front Med (Lausanne). 2022;9:904604. 19. Correia FF, Ramos I, Lopes B, et al. Topometric and tomographic indices for the diagnosis of keratoconus. Int J Kerat Ect Cor Dis. 2012;1(2):92-9. 20. Ambrósio R Jr. Enhancing ectasia screening. CRST Global Europe Edition. crstodayeurope.com/articles/2009-nov/crsteuro1109_07-php. Published November 2009. Accessed February 1, 2024. |
