Erectile dysfunction (ED) affects up to 30 million men in the United States, including half of all men ages 40 to 70.1 Some 7% of men ages 18 to 29 have some form of ED, as do 18% of men ages 50 to 59.2 So, its no wonder that Viagra (sildenafil, Pfizer), the so-called little blue pill, is one of the worlds best-selling pharmaceutical agents.
However, several studies have associated the drug with nonarteritic anterior ischemic optic neuropathy (NAION).3-9 In June, Pfizer agreed to include the report of NAION on the Viagra label, even though the company said its own review of 13,000 patients found no evidence that NAION occurred more frequently in men taking Viagra than in men of similar age and health who did not take the drug.
Still, optometrists must know how sildenafil works and be aware of potential adverse ocular side effects. Here, well discuss the drugs mechanism of action and possible adverse effects.
ED Defined
Erectile dysfunction is defined as the inability to achieve or maintain an erection sufficient for satisfactory sexual performance.10 While not life threatening, ED may result in a withdrawal from sexual intimacy and a reduced quality of life.11
The etiology of ED typically involves both organic and psychogenic factors.12 Almost any disease that alters the vascular, nervous or endocrine systemsincluding diabetes mellitus, hypertension, heart disease and depressioncan increase the risk of developing ED. Smoking is another risk factor. Also, the risk of ED dramatically increases with age.11
Penile erections involve the coordination of psychological, neurological, endocrine, vascular and muscular components. Tumescence, the vascular filling of the corpus cavernosa (cavernous bodies) of the penis, relies on neural and hormonal mechanisms that operate at various levels of the neural axis. The brain gathers information from a particular stimulus (touch, smell or visual) and sends that information to the base of the spine. There, primary nerve fibers that connect to the penis regulate blood flow during and after an erection.
Specifically, blood flow regulation depends on the relaxation and constriction of the smooth muscle of the cavernous bodies, which react via nitric oxide (NO) and cyclic guanosine monophosphate (cGMP). During sexual stimulation, the NO-cGMP pathway facilitates the relaxation of smooth muscle, thus increasing blood flow while closing venous drainage channels. The cavernous bodies become full and rigid, resulting in an erection.12
Therapies for ED include sexual counseling, external vacuum devices, vasoactive injection therapies, penile implants and oral medications such as sildenafil. Newer, similar medications include Levitra (vardenafil hydrochloride, Bayer Pharmaceuticals/GlaxoSmithKline) and Cialis (tadalafil, Eli Lilly).
Viagras Action
Sildenafil itself does not cause an erection. Rather, it inhibits phosphodiesterase-5 (PDE5), an enzyme that degrades cGMP, thus increasing intracellular levels of cGMP. This, in turn, promotes relaxation of the smooth muscle of the penis to enhance erectile function.
The standard recommended starting dose is 25mg to 50mg. The dose may be increased to 100mg if needed, although higher doses have an increased incidence of side effects with little gain in efficacy. Patients are typically instructed not to use sildenafil more than once in any 24-hour period and not to use the drug more than two or three times per week.13 Sildenafil reaches a peak plasma concentration between two and four hours.
Because sildenafil potentiates vasodilation, the concomitant use of any nitrates is an absolute contraindication for its use, as these increase the possibility of abrupt and potentially serious hypotension.13 Also, because sildenafil is metabolized predominantly by the cytochrome P450 3A4 isoenzyme, patients who take medications that inhibit this pathway (erythromycin, ketoconazole and cimetidine) should not take sildenafil or should at least lower their dosage and/or frequency of use.14
Although sildenafil primarily affects PDE5, most potential side effects occur because the drug has a slight effect on other phosphodiesterases throughout the body, including those in the brain and cardiac tissue. The most common side effects of sildenafil include headache, flushing, dyspepsia, nasal congestion and visual disturbances.13
Serious cardiovascular, cerebrovascular and vascular eventsincluding myocardial infarction, sudden cardiac death, ventricular arrhythmia, cerebrovascular hemorrhage, transient ischemic attack, hypertension, subarachnoid and intracerebral hemorrhages, and pulmonary hemorrhageare possible, though rare, side effects.15 The FDA has concluded that it is not possible to determine whether these events are directly related to Viagra, sexual activity, underlying cardiovascular disease, a combination of these factors or other factors.16
Ocular Side Effects
Ocular side effects of sildenafil have been well documented. The most prominent: complaints of a bluish tinge to vision, increased light sensitivity and halos.11,17 The incidence of these visual symptoms is infrequent at low doses but may be as high as 50% at 200mg.18
The mechanism for this phenomenon remains unknown. One theory: Sildenafil has up to 10% effectiveness against phosphodiesterase-6, an enzyme localized to the photoreceptors in the retina. This enzyme is important in transduction, the process in which light energy is converted to a neural signal. Because of the action against PDE6, alterations in cGMP within the cone photoreceptors may be responsible for these visual side effects.13
Higher doses of Viagra (>200mg) have been reported to cause transient visual changes, slight electroretinogram changes and subtle color-vision changes.13,19-21 There is no significant evidence that sildenafil affects visual acuity, visual field, IOP or visual evoked potentials.22,23
NAION
More serious ocular side effects that have irreversible visual complications also have been linked with sildenafil. Since 1999, more than 20 documented cases of nonarteritic anterior ischemic optic neuropathy (NAION) occurred among individuals following sildenafil ingestion.3-9
 |
|
1. Patients who have NAION may initially notice visual field loss; altitudinal defects, as seen here, are most common. |
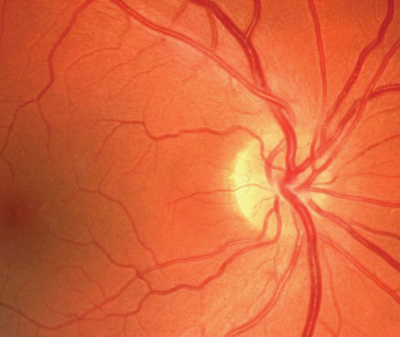
A disc at riska crowded, small optic nerve head that has a small physiologic cup, abnormal branching of the central vessels and full nerve fiber bundles obscuring the disc marginis the typical optic nerve head seen in NAION and is almost always seen in the fellow eye (figure 4).24 Visual acuity may vary from 20/20 to a marked loss of vision, depending on which part of the optic nerve head is involved.
 |
 |
|
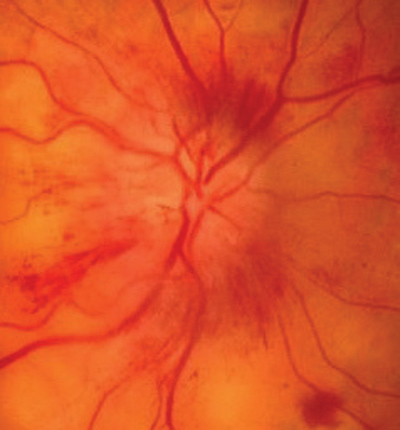
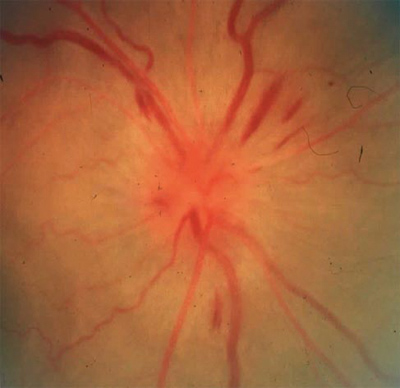
2, 3. Clinical examination of NAION reveals a diffuse or focally swollen optic disc, and multiple flame-shaped hemorrhages surrounding the disc are usually present. |
Structural factors of a disc at risk and subsequent alterations to perfusion pressure in the peripheral branches of the posterior ciliary arteries lead to microvascular ischemia.28 This ischemia, which occurs in the capillaries, causes axoplasmic stasis and edema of the optic nerve head. Risk is significantly increased in older patients, as their capillaries often are already compromised, potentially increasing the level of ischemia.
The role of sildenafil in NAION is unknown, but reports suggest that the effect on blood pressure through the NO-cGMP pathway may be responsible.3-5,21,22,29-31 Just as NO can regulate blood pressure through vasodilation, NO may also dilate blood vessels around the optic nerve head and influence its perfusion, subsequently interfering with the autoregulation of ocular blood flow.5,22,29-31
The circulation of the optic disc, peripapillary choroid and choroid depends upon the difference in perfusion pressure of the posterior ciliary arteries and IOP.28 If sildenafil accentuates hypotension enough, the perfusion pressure in the posterior ciliary arteries may decrease and cause an oxygen imbalance, and ultimately an ischemic optic nerve head. This is a similar pathophysiological process to that of nocturnal arterial hypotension, which may cause decreased perfusion to the optic disc.32 If the optic nerve head was already predisposed to ischemia by an anatomic disc at risk configuration, it becomes even more plausible that NAION may develop.
 |
|
4. A disc at risk is the typical optic nerve head seen in NAION. |
Other Ocular Complications
Much less prevalent yet serious ocular complications possibly associated with sildenafil usage have occurred. These include one reported case of a third-nerve palsy, (presumably from third-nerve ischemia), one reported case of central serous chorioretinopathy, two reported cases of serous macular detachments (presumably from choroidal ischemia), and one reported case of branch retinal artery occlusion (presumably secondary to cardiac ischemia that lead to arrhythmia and subsequent embolus formation).33-37 As with NAION, a hypotensive ischemic event secondary to the NO effect on various organs was suspected in each of these cases.
The ocular findings associated with sildenafil usage may have important implications for other anti-ED medications. Recently, two cases of NAION have been reported in individuals after they used Cialis.38,39 Tadalafil acts similarly to sildenafil, but is more specific for PDE5 and lasts up to 36 hours. Although we cannot positively associate tadalafil and NAION based solely on these two cases, they should raise our suspicion. To date, no such cases have been reported with Levitra, a similar, long-lasting PDE5 inhibitor.
The O.D.s Role
Although it is sensitive information patients would often rather not discuss with their eye doctors, it is important to ask every male patient about the use of ED medications. By explaining why it is important for you to know and briefly describing the possible ocular complications associated with these medications, patients may be more willing to disclose this information.
Pay careful attention to patients who are being treated for ED with one of the PDE5 inhibitors because most are already at a higher risk of developing a vascular event secondary to age. If nothing else, when a patient presents with signs and symptoms of NAION, a complete review of medications, including specific questions regarding sildenafil usage, is imperative.
Inform your patients about the potential risks of sildenafil. Pay particular attention to patients who have a history of monocular NAION as sildenafil usage may increase the risk of NAION in the fellow eye.
If you note ocular ischemia in patients taking sildenafil, report it to the National Registry of Drug-Induced Ocular Side Effects (http://piodr.sterling.net) for further evaluation.
Viagra has been a well-known treatment option for men who suffer from erectile dysfunction. O.D.s must be aware of potential adverse ocular side effects, recognize and treat sildenafil-related conditions, and help patients make informed decisions regarding its use.
Dr. Duszak practices at the Philadelphia Veterans Affairs Medical Center, the Nemours Health Clinic in Wilmington, Del., and a private-practice in Philadelphia. He has lectured on the ocular side effects of Viagra.
1. Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: prevalence and predictors. JAMA 1999 Feb; 281(6):537-44.
2. Feldman HA, Goldstein I, Hatzichristou DG, et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol 1994 Jan; 151(1):54-61.
3. Pomeranz HD, Bhavsar AR. Nonarteritic ischemic optic neuropathy developing soon after use of sildenafil (Viagra): a report of seven new cases. J Neuroophthalmol 2005 Mar; 25(1):9-13.
4. Egan R, Pomeranz H. Sildenafil (Viagra) associated anterior ischemic optic neuropathy. Arch Ophthalmol 2000 Feb;118(2):291-2.
5. Pomeranz HD, Smith KH, Hart WM Jr, Egan RA. Sildenafil-associated nonarteritic anterior ischemic optic neuropathy. Ophthalmology 2002 Mar;109(3):584-7.
6. Cunningham AV, Smith KH. Anterior ischemic optic neuropathy associated with Viagra. J Neuroophthalmol 2001 Mar;21(1):22-5.
7. Boshier A, Pambakian N, Shakir SA. A case of nonarteritic ischemic optic neuropathy (NAION) in a male patient taking sildenafil. Int J Clin Pharmacol Ther 2002 Sep;40(9):422-3.
8. Pomeranz H. Sildenafil (Viagra) associated NAION: additional cases. 29th Annual North American Neuro-Ophthalmology Society Meeting. Presentation No. 108. Snowbird, Utah 2003.
9. Akash R, Hrishikesh D, Amith P, Sabah S. Case report: association of combined nonarteritic anterior ischemic optic neuropathy (NAION) and obstruction of cilioretinal artery with overdose of Viagra. J Ocular Pharmacol Ther 2005 Aug; 21(4):315-7.
10. NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993 Jul 7;270(1): 83-90.
11. Fink HA, Mac Donald R, Rutks IR, et al. Sildenafil for male erectile dysfunction: a systematic review and meta-analysis. Arch Intern Med 2002 Jun 24;162(12):1349-60.
12. Brossman SA, Leslie SW. Erectile dysfunction. Emedicine.com 2004. www.emedicine.com/med/topic3023.htm.
13. Marmor MF, Kessler R. Sildenafil (Viagra) and ophthalmology. Surv Ophthalmol 1999 Sep-Oct;44(2):153-62.
14. Zusman RM, Morales A, Glasser DB, Osterloh IH. Overall cardiovascular profile of sildenafil citrate. Am J Cardiol 1999 Mar 4;83(5A):35c-44c.
15. Physicians Desk Reference. 56th ed. Montvale, N.J.: Medical Economics 2001:2534-7.
16. Food and Drug Administration Joint Clinical Review. Study 148-228: An open, randomized, single oral dose, four-way crossover study to determine the dose proportionality of the pharmacokinetics of sildenafil in healthy male volunteers over the dose range 25mg to 200mg:167-9.
17. Gabrieli CB, Regine F, Vingolo EM, et al. Subjective visual halos after sildenafil (Viagra) administration: electroretinographic evaluation. Ophthalmology 2001 May; 108(5):877-81.
18. Laties A, Ellis P, Mollon JD. The effects of sildenafil citrate (Viagra) on color discrimination in volunteers and patients with erectile dysfunction (abstract). Invest Ophthalmol Vis Sci 1999;40:S693(supplement).
19. Kretschman U, Gockeln R, Meschi M, et al. Short time influences of sildenafil on visual function (abstract). Invest Ophthalmol Vis Sci 1999;40:S7666(supplement).
20. Vobig MA, Klotz T, Staak M, et al. Retinal side-effects of sildenafil. Lancet 1999 Jan;353(9150):375.
21. Zrenner E. No cause for alarm over retinal side-effects of sildenafil. Lancet 1999 Jan 30;353(9150):340-1.
22. Grunwald JE, Siu KK, Jacob SS, Dupont J. Effect of sildenafil citrate (Viagra) on the ocular circulation. Am J Ophthalmol 2001 Jun;131(6):751-5.
23. Ermis SS, Inan UU, Samli M, Ozturk F. Acute effects of sildenafil on Humphrey visual field and intraocular pressure. Int Ophthalmol 2004 Mar;25(2):69-72.
24. Burde RM. Optic disk risk factors for nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol 1993 Dec 15;116(6):759-64.
25. Characteristics of patients with nonarteritic anterior ischemic optic neuropathy eligible for the Ischemic Optic Neuropathy Decompression Trial. Arch Ophthalmol 1996 Nov;114(11):1366-74.
26. Hattenhauer MG, Leavitt JA, Hodge DO, et al. Incidence of nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol 1997 Jan;123(1):103-7.
27. Johnson LN, Arnold AC. Incidence of nonarteritic and arteritic anterior ischemic optic neuropathy. Population-based study in the state of Missouri and Los Angeles County, California. J Neuroophthalmol 1994 Mar;14(1):38-44.
28. Hayreh SS. Anterior ischemic optic neuropathy. I. Terminology and pathogenesis. Br J Ophthalmol 1974 Dec;58(12): 955-63.
29. Sponsel WE, Paris G, Sandoval SS, et al. Sildenafil and ocular perfusion. N Engl J Med 2000 Jun 1;342(22):1680.
30. Koksal M, Ozdemir H, Kargi S, et al. The effects of sildenafil on ocular blood flow. Acta Ophthalmol Scand 2005 Jun;83(3):355-9.
31. McCulley TJ, Luu JK, Marmor MF, Feuer WJ. Effects of sildenafil citrate (Viagra) on choroidal congestion. Ophthalmologica 2002 Nov-Dec;216(6):455-8.
32. Hayreh SS, Zimmerman MB, Podhajsky P, Alward WL. Nocturnal arterial hypotension and its role in optic nerve head and ocular ischemic disorders. Am J Ophthalmol 1994 May 15;117(5):603-24.
33. Donahue SP, Taylor RJ. Pupil-sparing third nerve palsy associated with sildenafil citrate (Viagra). Am J Ophthalmol 1998 Sep;126(3):476-7.
34. Allibhai ZA, Gale JS, Sheidow TS. Central serous chorioretinopathy in a patient taking sildenafil citrate. Ophthalmic Surg Lasers Imaging 2004 Mar-Apr;35(2):165-7.
35. Sinha S, Pathak-Ray V, Ahluwalia H, Morgan JE. Viagra or what? Eye 2004 Apr;18(4):446-8.
36. Quiram P, Dumars S, Parwar B, Sarraf D. Viagra-associated serous macular detachment. Graefes Arch Clin Exp Ophthalmol 2005 Apr;243(4):339-44.
37. Tripathi A, ODonnell NP. Branch retinal artery occlusion; another complication of sildenafil. Br J Ophthalmol 2000 Aug;84(8):934-5.
38. Escaravage GK, Wright JD, Givre SJ. Tadalafil associated with anterior ischemic optic neuropathy. Arch Ophthalmol 2005 Mar;123(3):399-400.
39. Bollinger K, Lee MS. Recurrent visual field defect and ischemic optic neuropathy associated with tadalafil rechallenge. Arch Ophthalmol 2005 Mar;123(3):400-1.
