 |
A 78-year-old Caucasian male was referred to our institute for evaluation. Past medical history was extensive, with a family history of cancer, which notably included the patient’s lung cancer diagnosis; he underwent resection one year prior with subsequent chemotherapy infusions every 21 days. Past ocular history included cataract surgery in both eyes over a decade ago. He was a cigarette smoker for many years and denied any history of illicit drug use.
Best-corrected visual acuity was 20/25 OD and OS. Confrontation visual fields were full to finger counting, extraocular motilities were full and pupils were equal in size without an afferent pupillary defect OU. IOP was 14mm Hg OD and 13mm Hg OS. Anterior segment exam revealed multiple pigmented iris lesions OU and posterior chamber intraocular lenses with clear posterior capsules OU. Fundus imaging is shown below.
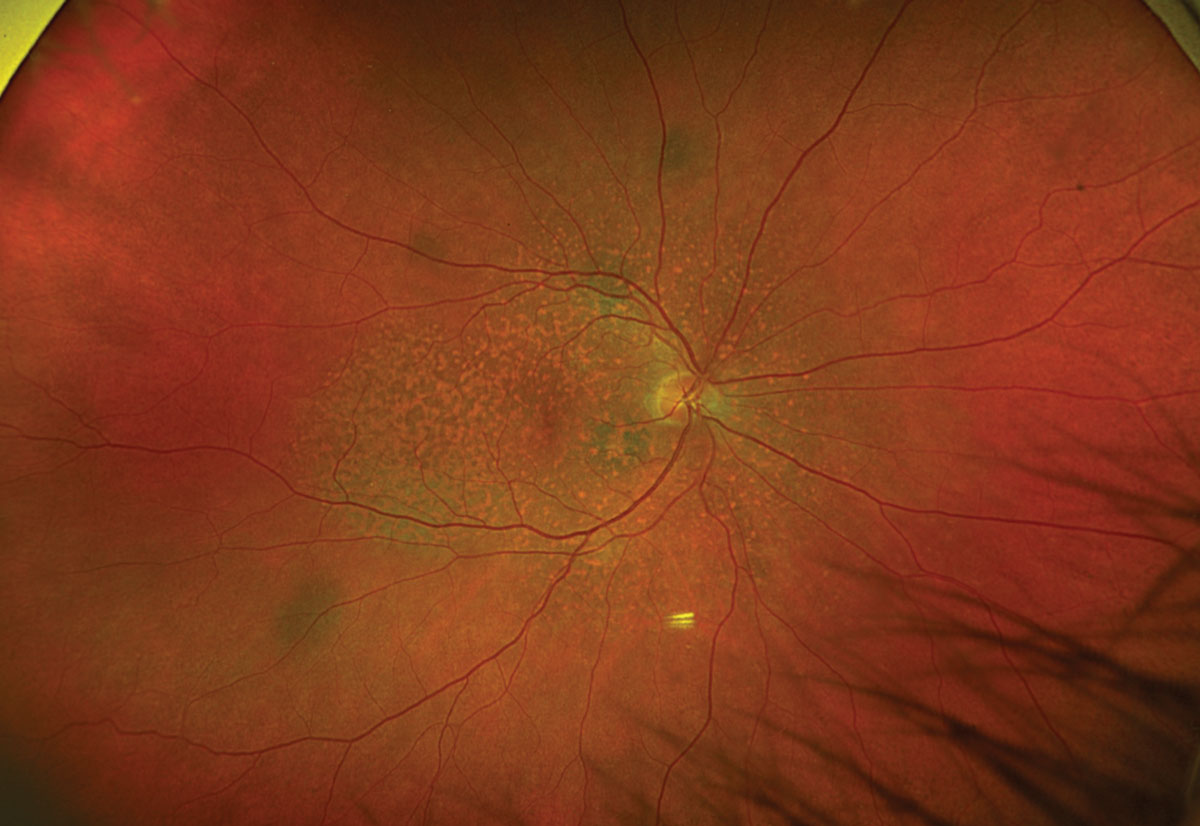 |
Fig. 1. Optos ultrawide fundus photograph of the right eye. Click image to enlarge. |
 |
|
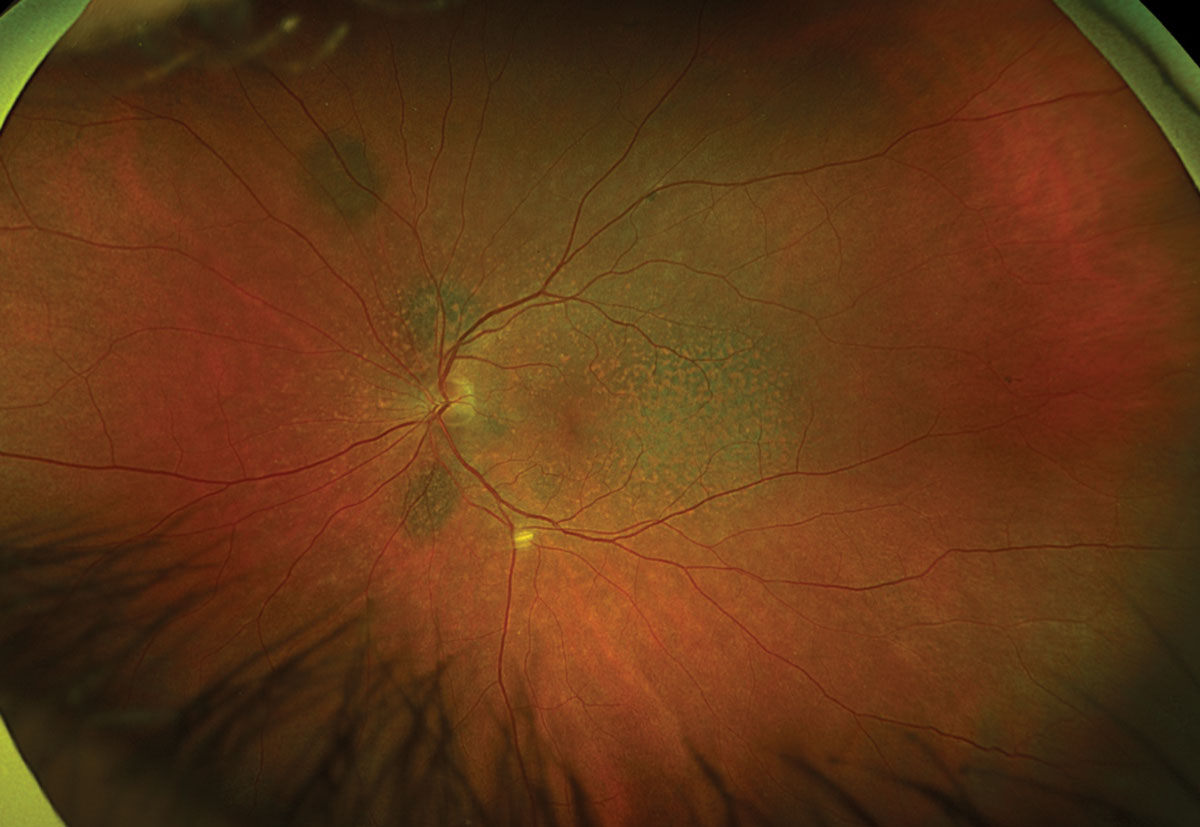
Fig. 2. Optos ultrawide fundus photograph of the left eye. Click image to enlarge. |
Take the Retina Quiz
1. Upon review of the images, all of the below are true except:
a. There are bilateral multifocal melanocytic lesions.
b. FAF displays diffusely stippled hypo- and hyperautofluorescence throughout the posterior pole OU.
c. OCT of the right eye demonstrates a thickened and homogeneously hyperreflective choroidal lesion in the nasal macula.
d. All of the above are true.
2. What is the most likely diagnosis?
a. Bilateral diffuse uveal melanocytic proliferation.
b. Choroidal metastases.
c. Uveal melanoma.
d. Uveal effusion syndrome.
3. Which of the following is NOT associated with vision loss in this condition?
a. Rapid development of cataracts.
b. Exudative retinal detachment.
c. Infiltrative optic neuropathy.
d. All of the above are associated with vision loss.
4. What is the most appropriate management for this patient?
a. Close observation.
b. High-dose oral corticosteroids.
c. Intravitreal injection of an anti-VEGF agent.
d. Rapid initiation of plasmapheresis.
5. Which of the following is true?
a. Breast cancer is the most common malignancy associated with this condition.
b. Diplopia is a common associated finding due to extraocular muscle infiltration.
c. The overall prognosis is poor and average survival is 19 months from the time of visual symptom onset.
d. All of the above.
Diagnosis
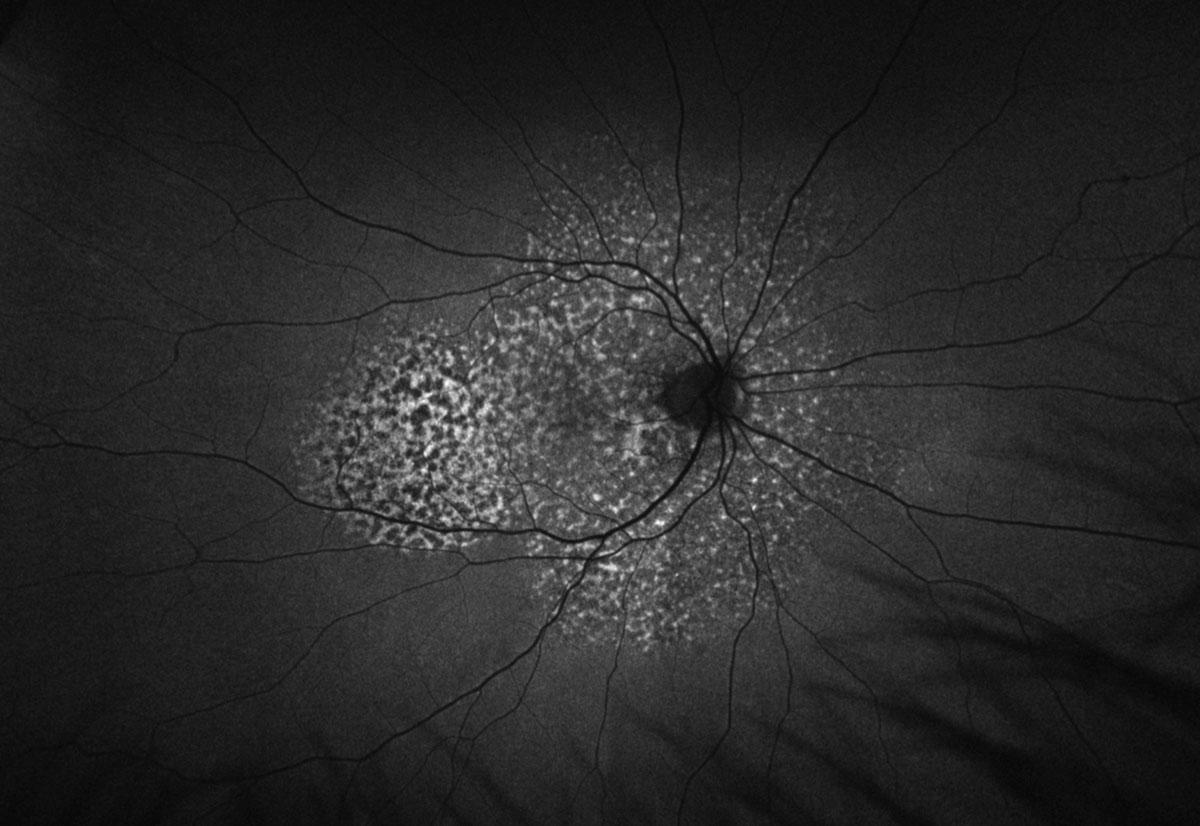
Fundus exam revealed diffuse multifocal reddish-orange patches creating a mottled reticular appearance of the posterior fundus with multiple scattered uveal melanocytic lesions OU. OCT showed irregular retinal pigment epithelial aggregations without subretinal fluid, as well as thickening and hyperreflectivity of the choroid corresponding with the melanocytic lesions. FAF revealed a characteristic “leopard spot” pattern consisting of diffuse areas of stippled hypo- and hyperautofluorescence. Angiography and echography were also obtained but not included due to space constraints. Fluorescein angiography displayed a distinct appearance of patchy early hypo- and hyperfluorescence corresponding to the findings on FAF, and indocyanine green angiography confirmed that the foci of melanocytic lesions were choroidal with discrete areas of hypocyanescence. This constellation of findings is consistent with the presentation of bilateral diffuse uveal melanocytic proliferation (BDUMP).
 |
|
Fig. 3. Optos FAF of the right eye. Click image to enlarge. |
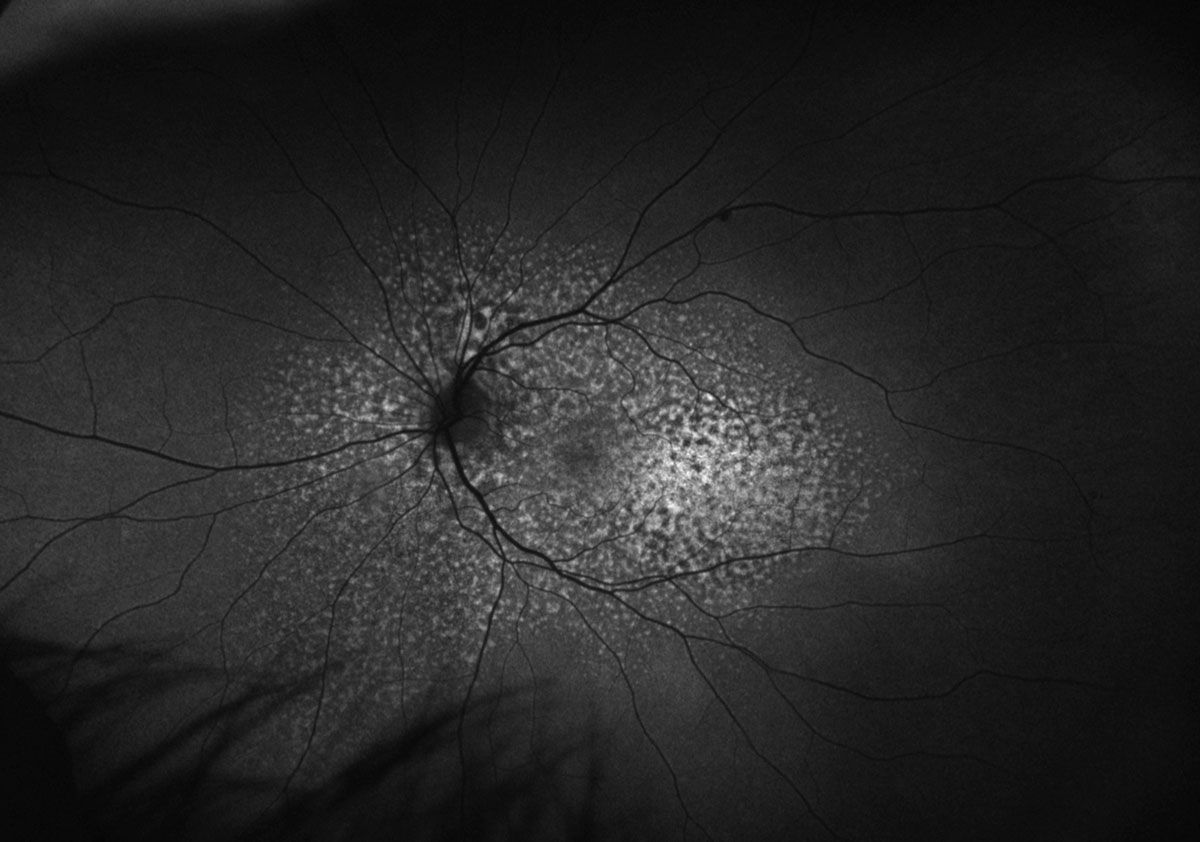 |
Fig. 4. Optos FAF of the left eye. Click image to enlarge. |
Discussion
While the exact pathophysiology of BDUMP is poorly understood due to its rarity, it is proposed that a serum borne tumor-produced factor—cultured melanocyte elongation and proliferation (CMEP)—leads to melanocyte proliferation and, thus, acquired melanocytic lesions of the uveal tract.5,8 It is unclear if both the systemic carcinoma of uveal proliferations are secondary to a common stimulus, if the CMEP is released by the systemic carcinoma or is there is another process involved.5-7 While BDUMP can be seen in association with any systemic malignancy, lung cancers are the most common in men, and reproductive tract cancers are the most common in women.9
These melanocytic lesions may infiltrate the iris, ciliary body and choroid, resulting in a breach in the blood-aqueous barrier and/or blood-retinal barrier via either direct or indirect mechanisms.7 Additionally, infiltration of the anterior uveal tract may induce metabolic dysfunction and secondary rapid cataract formation.5-7 In 1990, five cardinal ocular signs were proposed:1
(1) Multiple round or oval subtle red patches at the level of the RPE in the posterior fundus.
(2) Multifocal areas of early hyperfluorescence corresponding with these patches.
(3) Development of multiple, slightly elevated, pigmented and nonpigmented uveal melanocytic tumors, as well as evidence of diffuse thickening of the uveal tract.
(4) Exudative retinal detachment.
(5) Rapid progression of cataracts.
Vision loss primarily occurs by rapid cataract progression or loss of retinal function. Loss of retinal function may take place by either chronic exudative retinal detachment and its sequelae or by presumed toxic or immune-mediated destruction to the retina and retinal pigment epithelium (RPE).5,7 Histopathology has revealed that the characteristic fundus appearance of reddish-orange patches is related to RPE depigmentation overlying diffuse uveal infiltration of hypopigmented melanocytic proliferations.6,7 This results in the reticular pattern that we refer to as leopard spots.
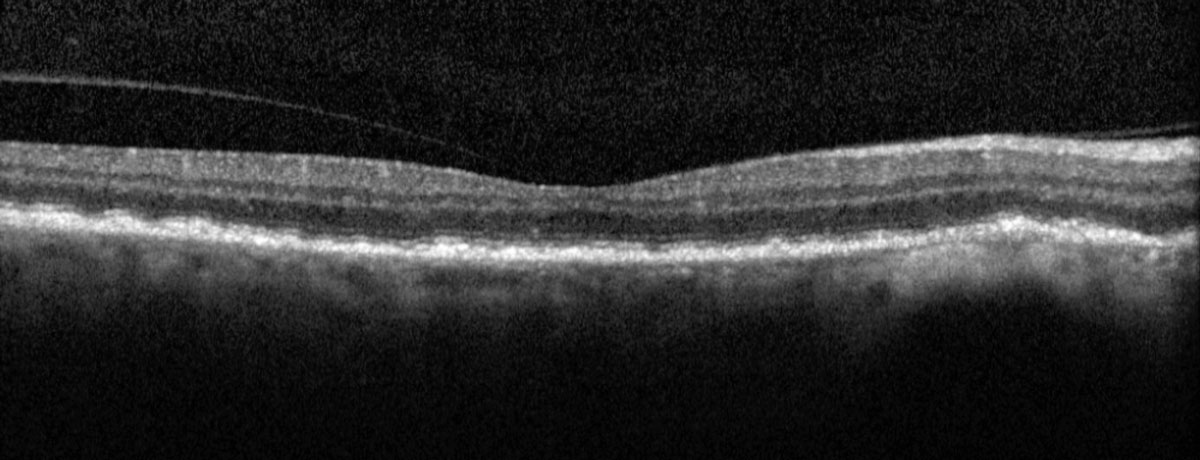 |
Fig. 5. Heidelberg macular OCT of the right eye. Click image to enlarge. |
Observation
In the absence of exudative retinal detachment, these patients are closely observed, with an emphasis often placed on addressing the primary malignancy.5,7-9 The serum-borne nature of CMEP factor suggests there may be a role for plasmapheresis, which has been shown effective in some cases.5,7-10 Furthermore, local/systemic corticosteroids and various forms of radiation/brachytherapy have been attempted without success.5,7-9
While data is scarce due to the rarity of the condition, the prognosis for patients with BDUMP is poor, as the average time to mortality after onset of visual symptoms is 19 months. Survival beyond seven years is rare; nearly all patients ultimately died from dissemination of the primary malignancy.1,5
This patient’s presentation of numerous bilateral melanocytic lesions of the anterior and posterior uveal tracts suggested that they were acquired. Furthermore, he had never been told of any “freckles” or pigmented lesions in the past. He was managed with close observation given the absence of exudative retinal detachment in both eyes. Concern for rapid cataract progression was not applicable given his pseudophakic status.
In summary, the discovery of bilateral acquired uveal melanocytic lesions should prompt investigation for a systemic malignant neoplasm if not already known to the patient.
Retina Quiz Answers
1: d, 2: a, 3: c, 4: a, 5: c
Drs. Aboumourad and Black currently practice at Bascom Palmer Eye Institute in Miami. Neither has any financial disclosures.
Dr. Dunbar is the director of optometric services and optometry residency supervisor at the Bascom Palmer Eye Institute at the University of Miami. He is a founding member of the Optometric Glaucoma Society and the Optometric Retina Society. Dr. Dunbar is a consultant for Carl Zeiss Meditec, Allergan, Regeneron and Genentech.
1. Gass JD, Gieser RG, Wilkinson CP, et al. Bilateral diffuse uveal melanocytic proliferation in patients with occult carcinoma. Arch Ophthalmol. 1990;108(4):527-33. 2. Saito W, Kase S, Yoshida K, et al. Bilateral diffuse uveal melanocytic proliferation in a patient with cancer-associated retinopathy. Am J Ophthalmol. 2005;140(5):942-5. 3. Machemer R. [On the pathogenesis of the flat malignant melanoma]. Klin Monbl Augenheilkd. 1966;148(5):641-52. 4. Barr CC, Zimmerman LE, Curtin VT, Font RL. Bilateral diffuse melanocytic uveal tumors associated with systemic malignant neoplasms. A recently recognized syndrome. Arch Ophthalmol. 1982;100(2):249-55. 5. Klemp K, Kiilgaard JF, Heegaard S, et al. Bilateral diffuse uveal melanocytic proliferation: Case report and literature review. Acta Ophthalmol. 2017;95(5):439-45. 6. Ryan SJ, Davis JL, Flynn HW, et al. Retina. Fifth ed. Saunders/Elsevier; 2013. 7. Agarwal A, Gass JDM. Gass’ Atlas of Macular Diseases. Fifth ed. Elsevier; 2011. 8. Miles SL, Niles RM, Pittock S, et al. A factor found in the IgG fraction of serum of patients with paraneoplastic bilateral diffuse uveal melanocytic proliferation causes proliferation of cultured human melanocytes. Retina. 2012;32(9):1959-66. 9. Moreno TA, Patel SN. Comprehensive review of treatments for bilateral diffuse uveal melanocytic proliferation: a focus on plasmaphereis. Int Ophthalmol Clin. 2017;57(1):177-94. 10. Kiryakoza LC, Diaz JD, Priluck J, et al. A case of bilateral diffuse uveal melanocytic proliferation in the setting of urothelial carcinoma of the ureter: a failed response to plasmapheresis. Ophthalmic Surg Lasers Imaging Retina. 2022;53(6):350-3. |
