 |
A 68-year-old gentleman presented to the ophthalmology department in consultation from the general medicine floor. He had been admitted for fever and fatigue but was confirmed as COVID negative. Following laboratory testing, it was confirmed he was in end-stage renal failure with poorly controlled hypertension and diabetes. The patient was a poor historian, not recalling that he had cataract surgery in both eyes in Columbia.
His chief complaint was decreased vision in the right eye of five days’ duration. The eye was red but not painful. He reported no allergies.
Clinical Findings
Examination was completed at the bedside. His best entering visual acuities were counting fingers at three feet OD and 20/40 uncorrected OS. There was no retinoscopic reflex in the right eye; the reflex in the left eye was normal, indicating gross emmetropia. His extraocular motilities were intact in both eyes but his confrontation field was restricted in the right eye, showing no peripheral awareness. The confrontation field in the left eye was normal. There was an afferent pupil defect, right eye.
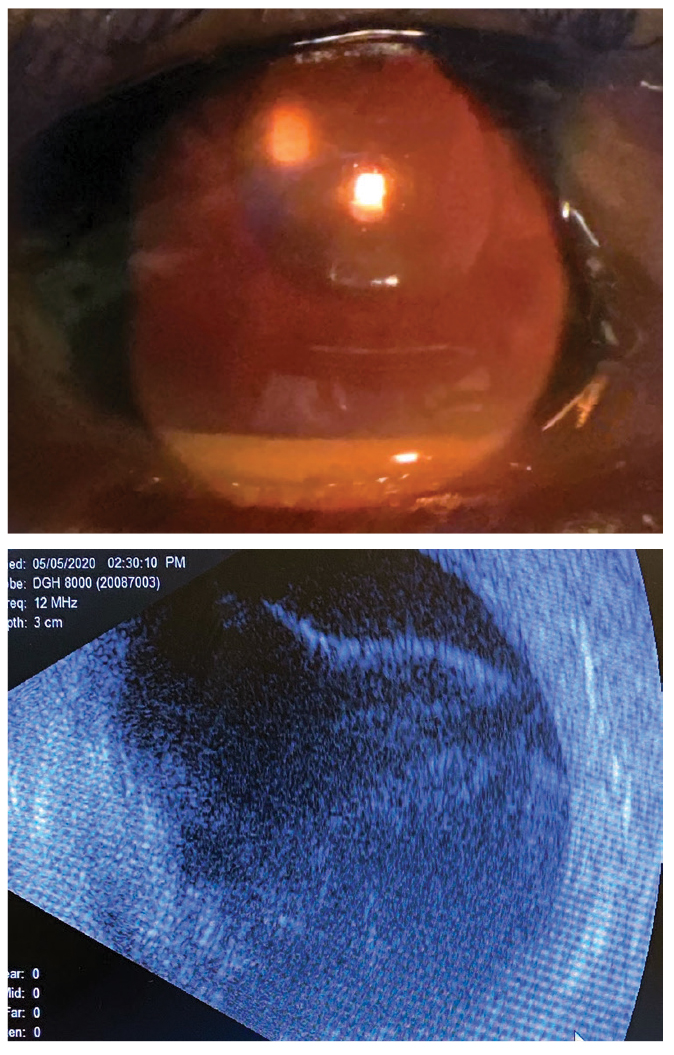
The gross examination of the anterior segment is demonstrated in the photograph. Intraocular pressures measured 12mm Hg in the right eye and 16mm Hg in the left by Tono-Pen. There was no evidence of rubeosis or ectropion uvea in either eye. Dilated examination demonstrated no view of the fundus OD and increased cupping (0.6) with mild nonproliferative diabetic retinopathy without macular edema OS.
 |
|
Slit lamp photo and ultrasound of our patient. Would you expect to see these presentations together? Click image to enlarge. |
Additional Testing
The patient was able to be transported to the office, where a proper slit lamp examination of the anterior segment demonstrated a hypopyon uveitis and dense vitritis OD. Binocular biomicroscopic indirect 90D lens examination was completed on both eyes. Anterior and posterior segment photography was completed. B-scan ultrasonography is demonstrated in the photograph and reveals a complete funnel-shaped retinal detachment, without evidence of serous retinal detachment or fibroproliferative debris.
Diagnosis
This month’s patient is experiencing endogenous endophthalmitis, seeded by confirmed sepsis of methicillin-resistant Staphylococcus aureus, with the incidental finding of complete rhegmatogenous retinal detachment OD.
Endophthalmitis is an infectious ocular inflammation of the intraocular cavity that can lead to irreversible visual loss.1-10 It may present acutely (within one to three days) after a surgical procedure or during a systemic infection, or in a delayed fashion many days after a surgical procedure (involving the eye or not) or systemic infection has passed.4,5 Acute endophthalmitis is a medical emergency.
Endophthalmitis is traditionally classified as exogenous (traumatic or post-surgical) or endogenous (arising from an internal cause), based on the transmission mode of the infectious source.1-5 The overall incidence of endophthalmitis following cataract surgery is low (0.04% to 0.4% of cases) but associated risk factors that can increase likelihood include intravenous drug use, diabetes mellitus, immune compromise, malignancy, prolonged hospital stay or intravenous antibiotic administration.3,7,8
Exogenous endophthalmitis occurs when infecting organisms enter the eye via an inoculation pathway. Most cases occur as a complication of cataract surgery, intravitreal injection (0.016% to 0.053% of all injections, injectable steroids > anti-VEGF drugs) or penetrating ocular trauma; however, cases have been reported after penetrating keratoplasty and invasive glaucoma surgeries.2,3
Endogenous endophthalmitis, by contrast, occurs when infectious organisms (bacteria or fungi) seed the eye hematogenously from a distant source of internal systemic infection.1 A complicating issue is that sepsis (bacteremia or fungemia) may be transient, with patients not manifesting ocular symptoms at the time systemic infection.2 This is permits endophthalmitis to present in a delayed fashion.2,4,5
Ocular Involvement
Since the ocular symptoms of endophthalmitis are non-specific (painful red eye, decreased vision, photophobia), early diagnosis relies on the alertness of the clinician to recognize the signs of the growing panuveitis and make the proper referral so that vitreoretinal pharmaco- and surgical therapy can be initiated. Early surgical intervention is the current trend in the management of endophthalmitis and is associated with the greatest potential to save function.1-10
The common pathogens in endophthalmitis vary by category.4,6 Coagulase-negative staphylococci are the most common causes of post-cataract endophthalmitis.4,6 Bacteria and viridans streptococci cause most cases of post-intravitreal anti-VEGF injection endophthalmitis.4,6 Bacillus cereus is a major cause of post-traumatic endophthalmitis.4,6 Staphylococcus aureus and streptococci are principal causes of endogenous endophthalmitis and endophthalmitis associated with endocarditis.4 Endogenous fungal endophthalmitis in hospitalized patients is usually caused by Candida species, particularly C. albicans.4,6 Klebsiella pneumoniae has been reported as a major source of endogenous endophthalmitis in association with liver abscess and in Asian countries.4,6
The signs and symptoms of endophthalmitis often include some variable uveitic findings such as ocular pain, photophobia and lacrimation, but these will depend upon the severity of the disease and the pain tolerance of the patient.1-13 Eyelid swelling has also been reported.9,10 The most common presenting symptoms are blurred vision and the new onset of floating spots.9 Visual acuity alteration is another highly variable sign, with some cases reporting 20/25 acuity and others reporting hand motion.9-13
The telltale sign is deep and substantial 360-degree conjunctival injection that does not blanch well with one drop of topical phenylephrine 2.5% ophthalmic solution. Clinically, the eye looks much more “angry” then circumstances call for. Often, there will be significant cells and flare, resulting in hypopyon (found in 80% of cases); however, unlike typical uveitis likely with this degree of inflammation, the inflammatory appearance may not match the level of pain (e.g., the inflammation observed is grade IV but the pain reported by the patient is grade I).1-14 If the source of the endophthalmitis is exogenous, there may be a well infiltrated wound site; if the cornea is involved, there may be edema and Descemet’s folds. Unless the case has been chronic and undiagnosed, synechial formation is rare even in the setting of a plasmoid aqueous humor.
Secondary to the anterior segment findings and vitritis, a retinoscopic reflex is often diminished or absent. Upon dilated fundus examination, there will be difficulty seeing posterior segment structures because the view is obstructed by some or all of the above. Chorioretinal lesions may be present, indicating chorioretinal inflammation and infection depending on the offending organism and the tissue it has invaded. The classic “string of pearls” sign is a linear arrangement of multiple round vitreoretinal inflammatory deposits that look like “snowballs” or resemble the pearls on a necklace. This is often seen in cases of retinal candidiasis with or without enodophthalmitis.9,10 If left untreated, chronic infection and inflammation may lead to globe perforation, blindness and loss of structure and organization (phthisis bulbi).9,10
Management Strategies
Endogenous endophthalmitis occurs when the infectious organism travels through the bloodstream and encounters the rich vascular choroidal network.10 There, nutrients and oxygen permit the organism to multiply. The growth eventually overtakes the cellular immune system and allows the organism to infiltrate the ocular tissues, triggering an aggressive inflammatory response in the retina and the vitreous.10
A diagnosis of endogenous endophthalmitis merits a systemic workup for the source of infection, although a substantial number of cases never yield a source (idiopathic endogenous endophthalmitis). The condition is most often associated with liver abscesses, sinus infection, endocarditis, meningitis or presence of catheters.1-16
B-scan ultrasonography should be completed to determine the extent and type of vitreous exudates present as well as measure the scleral thickness and examine the choroid for abscess and rule out retinal detachment (serous presumed).16 Computerized tomography (CT) scans of the orbit can rule out any orbital involvement. Other investigations such as complete blood count with differential and platelets, urinalysis, chest X-ray, ultrasound of the abdomen, CT or the abdomen, electro-echocardiography and Gallium scan are necessary to pursue identification of the systemic source of infection.1-14
Endophthalmitis of any kind—acute, delayed, exogenous, endogenous—is an ocular emergency requiring immediate referral to a retina specialist.1-11 Visual outcome is highly dependent on the causative organism, with any streptococci causing the worst outcomes, while coagulase-negative staphylococci cause milder cases.2,13 Overall, approximately half of eyes affected by post-cataract endophthalmitis do not regain a visual acuity of 20/40 or better, and 10% will lose useful vision (5/200 or worse).11,13
First aid may include topical cycloplegia with atropine 1% QD-TID, topical steroid therapy QID and topical antibiotic therapy QID with a topical antibiotic/steroidal combination ointment at bed.
While the literature recognizes that systemic antibiotics used to treat the underlying cause can achieve therapeutic levels in the eye assisted by a disrupted blood/ocular barrier, systemic agents are supplemented with intravitreal antimicrobials. Today, early vitrectomy may be considered by some retina specialists because new mechanical technologies (e.g., smaller instruments, faster cutters, transconjunctival approach, wider field of view) have permitted advancements in both the safety and the execution of the procedure.15
Classically, the Endophthalmitis Vitrectomy Study (EVS) concluded there was no advantage to vitrectomy for cases with prominent non-resolving vitreous involvement and entering visual acuity of light perception.11,15 The reason for a reluctance to doing vitrectomy was that, historically, while vitrectomized eyes were three times more likely to retain useful vision compared to those not receiving vitrectomy (offloading of a substantial microorganism load from the system, permitting treatment to be more effective), they were also more likely to encounter complications, which resulted in poor outcomes with increased rates of enucleation.11,15 Today, because of advancements in both instrumentation and technique, along with the advantage of collecting a specimen culture for anything aspirated during the procedure, the EVS guidelines are being reevaluated.15
Intravitreal administration of medications remains a staple of care: in bacterial cases, vancomycin (1mg/0.1mL) and ceftazidime (2.25mg/0.1mL) are the relied upon medications. Amikacin (0.4mg/0.1mL) and clindamycin (1.0mg/0.1mL) are alternatives for penicillin-allergic patients.1-14 Ciprofloxacin and the aminoglycosides are also often considered.1-15 Amphotericin-B (5-10μg/0.1mL) and less frequently voriconazole (100μg/0.1mL) are options for fungal cases.1-15
The systemic treatment is typically continued for at least three to four weeks after the ocular intervention but can be titrated shorter or longer as the extraocular infection dictates.
Dr. Gurwood is a professor of clinical sciences at The Eye Institute of the Pennsylvania College of Optometry at Salus University. He is a co-chief of Primary Care Suite 3. He is attending medical staff in the department of ophthalmology at Albert Einstein Medical Center, Philadelphia. He has no financial interests to disclose.
|
1. Sheu SJ. Endophthalmitis. Korean J Ophthalmol. 2017;31(4):283‐9. 2. Durand ML. Bacterial and fungal endophthalmitis. Clin Microbiol Rev. 2017;30(3):597‐613. 3. Relhan N, Forster RK, Flynn HW Jr. Endophthalmitis: then and now. Am J Ophthalmol. 2018;187(3):xx‐xxvii. 4. Vaziri K, Schwartz SG, Kishor K, Flynn HW Jr. Endophthalmitis: state of the art. Clin Ophthalmol. 2015;9(1):95‐108. 5. Armesto E, Cubillas M, Antón S. Bacterial endogenous endophthalmitis after colonoscopy. Rev Esp Enferm Dig. 2018;110(9):601. 6. Teweldemedhin M, Gebreyesus H, Atsbaha AH, et al. Bacterial profile of ocular infections: a systematic review. BMC Ophthalmol. 2017;17(1):212. 7. Ness T, Pelz K, Hansen LL. Endogenous endophthalmitis: microorganisms, disposition and prognosis. Acta Ophthalmol Scand. 2007;85(8):852‐6. 8. Tirpack AR, Duker JS, Baumal CR. An outbreak of endogenous fungal endophthalmitis among intravenous drug abusers in New England. JAMA Ophthalmol. 2017;135(6):534‐40. 9. Kernt M, Kampik A. Endophthalmitis: pathogenesis, clinical presentation, management and perspectives. Clin Ophthalmol. 2010;4(3): 121-35. 10. Chee SP, Jap A. Endogenous endophthalmitis. Curr Opin Ophthalmol. 2001;12(6):464-70. 11. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Endophthalmitis Vitrectomy Study Group. Arch Ophthalmol. 1995;113(12):1479‐96. 12. Forster RK. The endophthalmitis vitrectomy study. Arch Ophthalmol. 1995;113(12):1555‐7. 13. Kim CH, Chen MF, Coleman AL. Adjunctive steroid therapy vs. antibiotics alone for acute endophthalmitis after intraocular procedure. Cochrane Database Syst Rev. 2017;2(2):CD012131. 14. Sadiq MA, Hassan M Nguyen QD. Endogenous endophthalmitis: diagnosis, management and prognosis. J Ophthalmic Inflamm Infect. 2015;5(11):32. 15. Grzybowski A, Turczynowska M, Kuhn F. The treatment of postoperative endophthalmitis: should we still follow the endophthalmitis vitrectomy study more than two decades after its publication? Acta Ophthalmol. 2018;96(5):e651‐4. 16. Kimura D, Sato T, Suzuki H, et al. A Case of Rhegmatogenous Retinal Detachment at Late Stage following Endogenous Bacterial Endophthalmitis. Case Rep Ophthalmol. 2017;8(2):334‐40. |
