 |
A 45-year-old well-educated Caucasian male presented for his first eye exam in a new state since moving across the country. His only complaint was slightly blurred vision at near in both eyes through his two-year-old scratched reading glasses. No significant eye or health problem was reported. He started wearing glasses after failing the vision screening in the first grade. His myopia increased for many decades, which required a new prescription every several years. He was advised previously by several ODs and MDs that he was developing minor peripheral retinal degeneration and that he should obtain emergent care if he experienced changes such as an increase in flashes, floaters, shadows, spots, cobwebs or curtains.
With a minor change in prescription, VA was correctable to 20/20 in each eye at distance and near. The dilated fundus exam revealed several patches of lattice degeneration in each eye without holes, tears or vitreal traction and a one-disc-diameter pigmented choroidal nevus that was sketched the same size as the optic disc in his right eye. The nevus was within the arcades and superior-temporal to the fovea. Fundus photos were reportedly taken.
 |
|
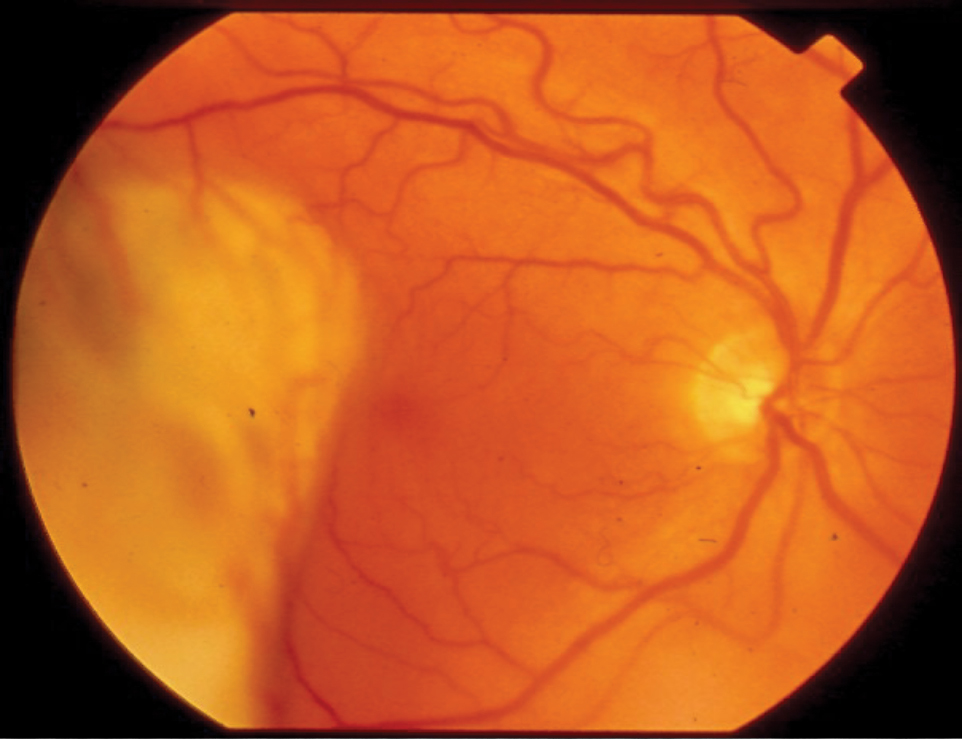
Choroidal nevus in the right eye from a different patient that corresponds quite closely to the description and sketch documented by the first eye clinician. Click image to enlarge. |
Glasses and daily contact lenses were prescribed. The patient was told about the lattice degeneration and to report any changes such as those discussed immediately because of the lattice degeneration in this 6D myope. A conversation about lattice degeneration sometimes resulting in peripheral retinal tears and the risk of retinal detachment was noted on the record.
When told about the small freckle in his right eye, the patient mentioned that none of the eye doctors he had seen over four decades mentioned seeing a small freckle. The eye doctor at this visit advised the patient that it was such a minor finding and present in about 10% of all patients that most eye doctors would not bother to alarm the patient with such a minor finding. The patient was scheduled for a comprehensive examination one year later.
About 10 months later, the patient began experiencing vague floaters and occasional flashes in his right eye. Erring on the side of caution, the patient called the group practice and was scheduled to be seen by their retina specialist the next morning. Best-corrected VA was 20/20 in each eye, and the symptomatic right eye was observed to have a temporal retinal detachment encroaching on the macula. However, a retinal tear was not observed, nor was the one-disc-diameter choroidal nevus as diagnosed nearly a year earlier. The fundus photos taken at the first visit were not commented on by the retina specialist.
You Be the Judge
In light of the facts presented thus far, consider the following questions:
- Was the freckle most likely a choroidal nevus that had been present for decades?
- Did the first eye clinician meet the existing standard of care? Would a like practitioner under like circumstances have performed any differently?
- Should the retinal detachment noted by the retina specialist have been reattached via surgery within a day?
- Since VA was 20/20 and the retinologist’s exam noted that the macula was clinically normal, would the diagnosis be a macula “on” retinal detachment, which has a better prognosis, or a macula “off” retinal detachment?
- Since the retina surgeon could not find a retinal tear, would you consider a non-rhegmatogenous retinal detachment as the diagnosis? The diagnosis of a non-rhegmatogenous retinal detachment often does not require retinal surgery.
- Since the retina specialist could not find a retinal tear responsible for the retinal detachment, should this surgeon have obtained a B-scan ultrasound prior to retinal surgery?
 |
|
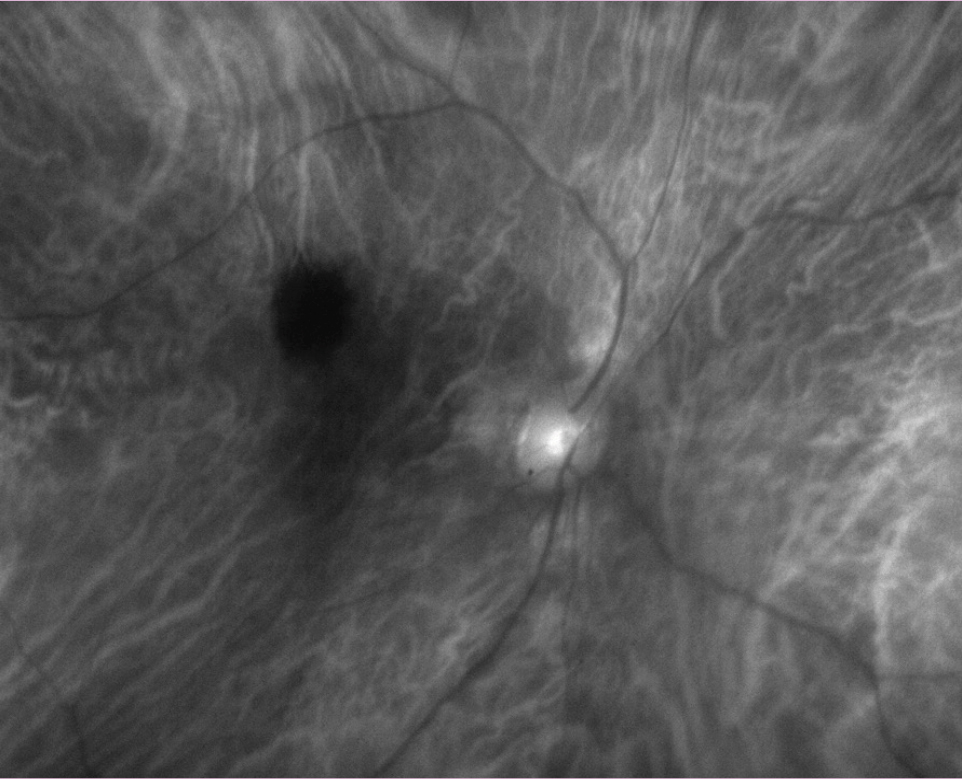
The actual fundus photo of the patient’s right eye taken that same day that patient was seen by the retinologist. Click image to enlarge. |
Follow-Up
The retinologist performed a B-scan ultrasound and observed a large mass under the retina. The patient was evaluated by an ophthalmic oncologist the next day and diagnosed with an amelanotic choroidal malignant melanoma and a secondary retinal detachment. The opinion of several ophthalmic oncologists was that the lesion observed a year earlier was not a benign choroidal nevus but a small, pigmented choroidal malignant melanoma. Occasionally, a small pigmented choroidal melanoma transforms into an amelanotic malignant melanoma when the lesion enlarges, such as in this case.
Proton beam irradiation was performed at a major teaching institution in a big city. The patient was also evaluated for any metastasis to another part of the body; no other lesions were found after an extensive work-up. The patient lost vision in the right eye but retained 20/20 VA and a normal field in the left eye.
The patient traveled to the National Eye Institute in the Washington, DC area and received experimental treatments that appeared to have been successful for at least several years. The patient and his family were optimistic that the myriad treatments were successful. However, the patient woke up one morning and observed a new pigmented lesion on his left inner thigh. He died several months later due to metastasis to several major organs.
 |
|
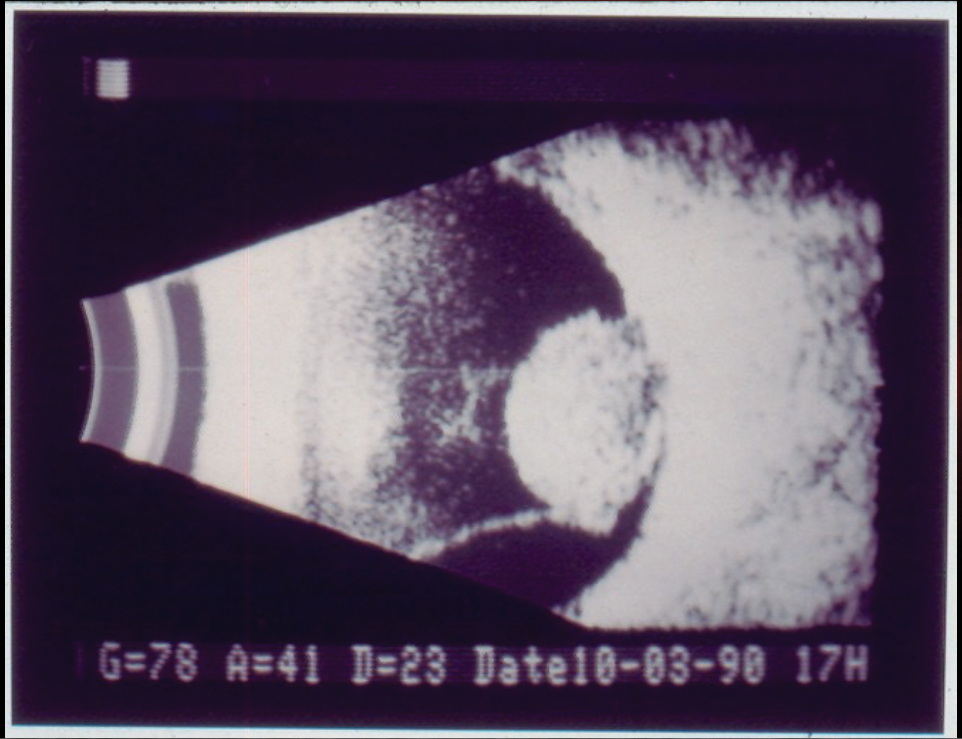
A B-scan ultrasound from a different but similar case demonstrating a large mass and secondary retinal detachment. Click image to enlarge. |
Malpractice Implications
One could argue that the first eye clinician should have taken seriously the patient’s comments on the first visit that no previous eye doctor ever mentioned a “freckle” in the patient’s right eye. This eye clinician could have obtained previous records, performed additional tests such as B-scan ultrasound and/or OCT and have the patient return in three months or so for a re-evaluation to determine if the lesion had increased in size, rather than waiting a year. According to the Blue Mountain Eye Study, choroidal nevi were present in 6.5% of the white population. In the United States, there are approximately only five cases of choroidal melanomas per year per million population.1 Approximately 20% of choroidal melanomas are amelanotic and hence represent only one case per year per million population.2,3 As a deduction, this unfortunate patient had only a one-in-a-million chance of developing an amelanotic malignant melanoma of the choroid.
The retinologist initially detected a retinal detachment but could not find a tear responsible for the detachment. A rhegmatogenous retinal detachment by definition has a tear and is typically treated with scleral buckles, vitrectomy and pneumatic retinopexy. If no tear is discovered, the diagnosis is non-rhegmatogenous retinal detachment, and a mass under the retina must be considered. A B-scan ultrasound should be obtained immediately, as it was in this case.
The first eye clinician testified that she took fundus photos in addition to her drawing. The retina surgeon testified that fundus photos were not included in the patient’s chart a year later. The surgeon correctly diagnosed the melanoma and immediately referred to an ophthalmic oncologist and hence met the standard of care. However, it has been conjectured that the retinologist did review the fundus photo slides from a year earlier, found them to be suggestive or indicative of a melanoma and decided to discard the photos. The fundus photos have never been found. Not surprisingly, the first eye clinician, the retinologist as well as the large group practice were all sued.
If you are ever faced with a similar situation, knowledge of this case will likely result in you assuming that the lesion was indeed new and required further evaluation. The retinologist appeared to have met the standard of care, but one could argue that he discarded essential evidence that would have suggested that the lesion diagnosed as a nevus a year earlier was really a small melanoma. The practice had poorly documented records with regards to fundus photos, and it could not be determined whether fundus photos were ever taken or even billed. The first eye clinician is no longer with the practice and the practice is under new management. After the patient’s death, the case was settled prior to a jury trial for several million dollars.
| NOTE: This article is one of a series based on actual lawsuits in which the author served as an expert witness or rendered an expert opinion. These cases are factual, but some details have been altered to preserve confidentiality. The article represents the authors’ opinion of acceptable standards of care and do not give legal or medical advice. Laws, standards and the outcome of cases can vary from place to place. Others’ opinions may differ; we welcome yours. |
Dr. Sherman is a Distinguished Teaching Professor at the SUNY State College of Optometry and editor-in-chief of Retina Revealed at www.retinarevealed.com. During his 52 years at SUNY, Dr. Sherman has published about 750 various manuscripts. He has also served as an expert witness in 400 malpractice cases, approximately equally split between plaintiff and defendant. Dr. Sherman has received support for Retina Revealed from Carl Zeiss Meditec, MacuHealth and Konan.
Dr. Bass is a Distinguished Teaching Professor at the SUNY College of Optometry and is an attending in the Retina Clinic of the University Eye Center. She has served as an expert witness in a significant number of malpractice cases, the majority in support of the defendant. She serves as a consultant for ProQR Therapeutics.
1.Sumich P, Mitchell P, Wang JJ. Choroidal nevi in a White population: The Blue Mountains Eye Study. Arch Ophthalmol. 1998;116(5):645-50. 2. Markiewicz A, Donizy P, Nowak M, et al. Amelanotic uveal melanomas evaluated by indirect ophthalmoscopy reveal better long-term prognosis than pigmented primary tumors-a single center experience. Cancers (Basel). 2022;14(11):2753. 3. Stuart K, Patel S. Amelanotic choroidal melanoma: a teaching case report. J Optometric Ed. 2021;46(2). |
